
Guidance on Planning for
Integration of Functional
Needs Support Services in
General Population Shelters
November 2010
2
This guidance was created for FEMA by
BCFS Health and Human Services, San Antonio, Texas; www.bcfs.net; 1-800-830-2246

Guidance on Planning for
Integration of Functional Needs
Support Services in General
Population Shelters
Contents
Page Section
7 1. Purpose
7 2. Disclaimer
8 3. Scope
8 3.1. Denition
8 3.2. FNSS Planning
9 3.3. Premise
10 3.4. Legal Foundation for FNSS Guidance
12 3.5. Legal Authorities and References
13 4. FNSS Guidance
15 4.1. Key Considerations in Planning for Shelter Set-Up
15 4.1.1. Planning in Advance for FNSS
16 4.1.2. Stakeholder Coordination
17 4.1.3. Planning Shelter Capacity
17 4.1.4. Identifying Shelter Sites/Facilities
18 4.1.5. Evaluating the Shelter

18 4.1.6. Selecting the Shelter
19 4.1.7. Equipping and Supplying the Shelter
21 4.1.8. Locating Services
23 4.1.9. Stafng the Shelter
24 4.1.10. Assessment Teams
25 4.1.11. Shelter Layout
25 4.1.12. Shelter Intake
27 4.2. Key Considerations in Planning for Shelter Operations
28 4.2.1. Dietary
28 4.2.2. Service Animals
30 4.2.3. Communication
31 4.2.4. Bathing and Toileting Needs
32 4.2.5. Quiet Area
32 4.2.6. Mental Health Services
32 4.2.7. Medical and Dental Services
34 4.2.8. Medication
35 4.2.9. Transportation Services
37 4.3. Key Considerations in Planning for Transition/Recovery
37 4.3.1. Transitioning Back to the Community
38 4.3.2. Closing the Shelter
40 5. Acronyms
41 6. Glossary
44 7. Operational Tools
45 8. Appendices
5
Acknowledgements
FNSS Review Panel Members that helped direct and
dene this guidance document
FEMA
• Mass Care Section
• Ofce of Disability Integration and Coordination
• Volunteer Agency Liaison
• Faith Based Ofce
• Ofce of Chief Council
• Region I
• Region VI
• Region X
HHS
• ESF 8 Ofce of the Assistant Secretary for Preparedness and Response ASPR
• ESF 6 Administration for Children and Families
DHS
• Ofce for Civil Rights and Civil Liberties
DOJ
• Disability Rights Section, Civil Rights Division
American Red Cross
• Direct Services
• Mass Care
• Disaster Health Services
National Council on Disability
National Council on Independent Living
National Disability Rights Network
Center for Disability and Health Policy
Rhode Island Department of Health
• Center for Emergency Preparedness & Response (CEPR)
Florida Statewide Disability Coordinator,
Division of Emergency Management
California Emergency Management Agency,
Ofce for Access and Functional Needs
6
7
Functional Needs
Support Services
Guidance on Planning for Integration of Functional
Needs Support Services in General Population
Shelters
1. Purpose
The purpose of this document is to provide planning guidance that can be incorporated into existing
shelter plans to State emergency managers and shelter planners to meet access and functional needs
in general population shelters. This document provides guidance to assist emergency managers
and shelter planners in understanding the requirements related to sheltering children and adults
with functional support needs in general population shelters. Functional Needs Support Services
(FNSS) and the guidance provided are designed to assist in the planning and resourcing of sheltering
operations whether government, NGO, faith- or private-based to meet the access and functional
needs of children and adults. These guidelines identify methods of achieving a lawful and equitable
program through the delivery of FNSS for children and adults.
2. Disclaimer
This guidance is not designed to establish local government as the single shelter operator or
establish a new “tier” of sheltering. It is not intended to establish new legal obligations, alter existing
obligations, or constitute a legal interpretation of the statutes that are the basis of the guidance
materials. The guidance is not meant to duplicate or cover all requirements found in existing or
potential shelter plans or SOP’s. This is simply a resource for integrating FNSS into the general
shelter planning process and/or existing documents. Listing an agency or organization’s processes/
procedures as an operational tool in this guidance does not constitute a recommendation or
endorsement of the resource. In addition, information presented in an operational tool may have been
summarized, modied and/or combined with other cited sources.
8
3. Scope
This guidance has been developed to support local, tribal, State and Federal governments to integrate
children and adults with and without disabilities who have access and functional needs into every
aspect of emergency shelter planning and response. It is intended to be used in conjunction with
general population shelter Standard Operating Procedures (SOP) to ensure that all shelter residents
benet equally from programs, services, and activities. It provides a context for FNSS integration in
light of other existing plans and describes a process to use in any planning effort. These guidelines
are scalable and can be applied to urban, suburban, and rural localities with multiple or limited
resources.
Children and adults with disabilities have the same right to services in general population shelters
as other residents. Emergency managers and shelter planners have the responsibility of planning
to ensure that sheltering services and facilities are accessible. The decisions made in the planning
process determine whether integration or segregation occurs during response. Although the FNSS
guidance is geared toward emergency managers and shelter planners, it is a document that can be
utilized as a shelter planning tool in local communities.
Throughout this document “State” is used to refer to a U.S. State, tribal government, U.S. territory
and the District of Columbia.
3.1. Denition
Functional Needs Support Services (FNSS) are dened as services that enable individuals to maintain
their independence in a general population shelter. FNSS includes:
• reasonable modication to policies, practices, and procedures
• durable medical equipment (DME)
• consumable medical supplies (CMS)
• personal assistance services (PAS)
• other goods and services as needed
Children and adults requiring FNSS may have physical, sensory, mental health, and cognitive and/or
intellectual disabilities affecting their ability to function independently without assistance.
Others that may benet from FNSS include women in late stages of pregnancy, elders, and people
needing bariatric equipment.
3.2. FNSS Planning
Planning for FNSS in general population shelters includes the development of mechanisms that
address the needs of children and adults in areas such as:
• Communication assistance and services when completing the shelter registration process and
other forms or processes involved in applying for emergency-related benets and services
including Federal, State, tribal, and local benets and services
• DME, CMS, and/or PAS that assist with activities of daily living
• Access to medications to maintain health, mental health, and function
• Available sleeping accommodations (e.g., the provision of universal/accessible cots or beds
and cribs; the placement, modication, or stabilization of cots or beds and cribs; the provision
and installation of privacy curtains)
• Access to orientation and way-nding for people who are blind or have low vision
9
• Assistance for individuals with cognitive and intellectual disabilities
• Auxiliary aids and services necessary to ensure effective communication for persons with
communication disabilities
• Access to an air-conditioned and/or heated environment (e.g. for those who cannot regulate
body temperature)
• Refrigeration for medications
• Availability of food and beverages appropriate for individuals with dietary restrictions (e.g.,
persons with diabetes or severe allergies to foods such as peanuts, dairy products and gluten)
• Providing food and supplies for service animals (e.g., dishes for food and water, arrangements
for the hygienic disposal of waste; and, if requested, portable kennels for containment)
• Access to transportation for individuals who may require a wheelchair-accessible vehicle,
individualized assistance, and the transportation of equipment required in a shelter because of
a disability
• Assistance locating, securing, and moving to post-disaster alternative housing, which includes
housing that is accommodating to the individual’s functional support needs (e.g., accessible
housing; housing with adequate space to accommodate DME; or housing located in close
proximity to public transportation, medical providers, job or educational facility, and/or retail
stores)
• Assistance with activities of daily living such as:
◦ eating
◦ taking medication
◦ dressing and undressing
◦ transferring to and from a wheelchair or other mobility aid
◦ walking
◦ stabilization
◦ bathing
◦ toileting
◦ communicating
3.3. Premise
Historically, resource gaps have existed in planning for and meeting access and functional needs
in general population shelters. Many times this has resulted in disparate treatment and the denial
of full and equal services. The intent of this planning guidance is to ensure that individuals are not
turned away from general population shelters and inappropriately placed in other environments (e.g.,
“special needs” shelters, institutions, nursing homes, and hotels and motels disconnected from other
support services). Addressing these gaps benets the entire community and maximizes resources.
10
3.4. Legal Foundation for FNSS Guidance
The Stafford Act and Post-Katrina Emergency Management Reform Act (PKEMRA), along with
Federal civil rights laws, mandate integration and equal opportunity for people with disabilities in
general population shelters.
To comply with Federal law, those involved in emergency management and shelter planning should
understand the concepts of accessibility and nondiscrimination and how they apply in emergencies.
The following are key nondiscrimination concepts applicable under Federal laws, and examples of
how these concepts apply to all phases of emergency management.
1. Self-Determination – People with disabilities are the most knowledgeable about their own
needs.
2. No “One-Size-Fits-All” – People with disabilities do not all require the same assistance and do
not all have the same needs.
• Many different types of disabilities affect people in different ways. Preparations should
be made for people with a variety of functional needs, including people who use mobility
aids, require medication or portable medical equipment, use service animals, need
information in alternate formats, or rely on a caregiver.
3. Equal Opportunity – People with disabilities must have the same opportunities to benet from
emergency programs, services, and activities as people without disabilities.
• Emergency recovery services and programs should be designed to provide equivalent
choices for people with disabilities as they do for people without disabilities. This
includes choices relating to short-term housing or other short- and long-term disaster
support services.
4. Inclusion – People with disabilities have the right to participate in and receive the benets of
emergency programs, services, and activities provided by governments, private businesses,
and nonprot organizations.
• Inclusion of people with various types of disabilities in planning, training, and evaluation
of programs and services will ensure that all people are given appropriate consideration
during emergencies.
5. Integration – Emergency programs, services, and activities typically must be provided in an
integrated setting.
• The provision of services such as sheltering, information intake for disaster services, and
short-term housing in integrated settings keeps people connected to their support system
and caregivers and avoids the need for disparate services facilities.
6. Physical Access – Emergency programs, services, and activities must be provided at locations
that all people can access, including people with disabilities.
• People with disabilities should be able to enter and use emergency facilities and access
the programs, services, and activities that are provided. Facilities typically required to be
accessible include: parking, drop-off areas, entrances and exits, security screening areas,
toilet rooms, bathing facilities, sleeping areas, dining facilities, areas where medical care
or human services are provided, and paths of travel to and from and between these areas.
7. Equal Access – People with disabilities must be able to access and benet from emergency
programs, services, and activities equal to the general population.
• Equal access applies to emergency preparedness, notication of emergencies, evacuation,
transportation, communication, shelter, distribution of supplies, food, rst aid, medical
care, housing, and application for and distribution of benets.
11
8. Effective Communication – People with disabilities must be given information that is
comparable in content and detail to that given to the general public. It must also be accessible,
understandable and timely.
• Auxiliary aids and services may be needed to ensure effective communication. These
resources may include pen and paper; sign language interpreters through on-site or video;
and interpretation aids for people who are deaf, deaf-blind, hard of hearing or have
speech impairments. People who are blind, deaf-blind, have low vision, or have cognitive
disabilities may need large print information or people to assist with reading and lling out
forms.
9. Program Modications – People with disabilities must have equal access to emergency
programs and services, which may entail modications to rules, policies, practices, and
procedures.
• Service staff may need to change the way questions are asked, provide reader assistance to
complete forms, or provide assistance in a more accessible location.
10. No Charge – People with disabilities may not be charged to cover the costs of measures
necessary to ensure equal access and nondiscriminatory treatment.
• Examples of accommodations provided without charge to the individual may include
ramps; cots modied to address disability-related needs; a visual alarm; grab bars;
additional storage space for medical equipment; lowered counters or shelves; Braille
and raised letter signage; a sign language interpreter; a message board; assistance in
completing forms or documents in Braille, large print or audio recording.
See FEMA: IV. Non-discrimination Principles of the Law; http://www.fema.gov/oer/reference/
principles.shtm
The Americans with Disabilities Act of 1990 (ADA), the Rehabilitation Act of 1973 (RA), and the
Fair Housing Act (FHA), their regulations and agency guidance, as well as State counterparts, among
others, dene the scope of FNSS. These hallmarks of equal opportunity for people with disabilities
include:
• The implementation and execution of a general policy of nondiscrimination on the basis of
disability
• Sheltering persons with disabilities in the most integrated setting appropriate to the needs of
the person, which in most cases is the same setting people without disabilities enjoy
• Reasonable modications of policies, practices, and procedures to ensure nondiscrimination,
with reasonableness judged in light of nondiscrimination principles applied in emergent
circumstances
• The provision of auxiliary aids and services to ensure effective communication, with primary
consideration of the aid or service given to the person with a disability
• Elimination of eligibility criteria, discriminatory administrative methods, paternalistic safety
requirements, and surcharges where discrimination results
• The selection of accessible sites for the location of general population emergency shelters,
the construction of architecturally compliant mass care shelters and elements, and required
physical modications to ensure program accessibility in existing facilities
12
3.5. Legal Authorities and References
ADA Best Practices Tool Kit for State and Local Governments, Chapter 7, Emergency Management
under Title II of the ADA (2007), Addenda 1-3, and the Introduction to Appendices 1 and 2 (Attached
as Exhibit 1); Titles II, III, and V of the Americans with Disabilities Act of 1990, 42 U.S.C. §§ 12101-
12103, 12131-12134, 12181-12188, and 12201-12213, as amended by the ADA Amendments Act
of 2008.
Nondiscrimination on the Basis of Disability in State and Local Government Services,
28 C.F.R. pt. 35.
Nondiscrimination on the Basis of Disability by Public Accommodations and in
Commercial Facilities, 28 C.F.R. pt. 36.
The Americans with Disabilities Act Title II Technical
Assistance Manual (1993) and Supplement (1994).
The Americans with Disabilities Act Title III
Technical Assistance Manual (1993) and Supplement (1994).
Section 504 of the Rehabilitation Act of 1973, 29 U.S.C. §§ 794, as amended.
Enforcement of
Nondiscrimination on the Basis of Handicap in Programs or Activities Conducted by the Federal
Emergency Management Agency, 44 C.F.R. pt. 16.
Enforcement of Nondiscrimination on the Basis
of Handicap in Programs or Activities Conducted by the Department of Justice, 28 C.F.R. pt. 39.
Nondiscrimination on the Basis of Handicap in Programs or Activities Receiving Federal Financial
Assistance, 45 C.F.R. pt. 84 (Department of Health and Human Services).
Nondiscrimination on
the Basis of Handicap in Programs or Activities Receiving Federal Financial Assistance, 34 C.F.R.
pt. 104 (Department of Education).
Nondiscrimination Based on Handicap in Federally Assisted
Programs and Activities of the Department of Housing and Urban Development, 24 C.F.R. pt. 8.
Title VIII of the Civil Rights Act of 1968 (“Fair Housing Act”), as amended, 42 U.S.C. §§ 3601-3631.
Discriminatory Conduct Under the Fair Housing Act, 24 C.F.R. pt. 100.
The Architectural Barriers Act of 1968, as amended, 42 U.S.C. §§ 4151-4157.
Construction and
Alteration of Public Buildings, 41 C.F.R. pt. 101-19.
The Homeland Security Act of 2002, 6 U.S.C. §§ 101-557, as amended.
The Robert T. Stafford Disaster Relief and Emergency Assistance Act, 42 U.S.C. §§ 5121-5206, as
amended.
Federal Disaster Assistance, 44 C.F.R. pt. 206.
The Post-Katrina Emergency Management Reform Act, 6 U.S.C. § 761(d), as amended.
Emergency managers and shelter planners are encouraged to investigate their applicable State laws.
13
4. FNSS Guidance
This document outlines common scenarios that general population shelter planners and operators may
encounter during emergencies and disasters, and presents guidance on providing an integrated, non-
dependent, nondiscriminatory environment, so people with and without disabilities may benet from
the same sheltering program.
The operational tools in this document are excerpts and examples taken from various agency and
jurisdictional documents throughout the United States. While they are not meant to dictate a State’s
policies or procedures, they do present ideas and practices that can be adapted to t each State’s
specic needs.
14
15
4.1. Key Considerations In
Planning For Shelter Set-Up
4.1.1. Planning in Advance for FNSS
The importance of advanced planning in developing and implementing FNSS in general population
shelters cannot be overstated. Throughout the document this principle will be repeated again and
again to emphasize that FNSS cannot wait to be identied and put into place once an emergency or
disaster occurs.
Often, it is assumed that during a disaster, children and adults requiring FNSS must be housed
in a medical special needs shelter. Children and adults with access and functional needs do not
necessarily have medical conditions and typically do not require the care that medical shelters
provide. Diverting to medical shelters can result in the separation of individuals with disabilities
from those associated with them such as family, friends, neighbors and caregivers. In addition,
inappropriate placement can jeopardize the health and safety of the entire community by creating
unnecessary surges on emergency medical resources.
A one-size-ts-all approach to shelter planning does not work. (See FEMA: IV.Non-discrimination
Principles of the Law; http://www.fema.gov/oer/reference/principles.shtm).
Under the Americans with Disabilities Act (ADA), children and adults with disabilities are entitled to
equal opportunity to participate in programs, services, and activities in the most integrated setting.
Historically, shelter facilities may not have met requirements under the Standards for Accessible
Design, 28 CFR Part 36 (adopted from ADA Architectural Guidelines). Newly constructed or
recently altered facilities are more likely to fully comply with standards for accessible design. The
decision to open a shelter that violates Federal laws and ADA standards brings with it signicant
challenges to appropriately and safely shelter children and adults with and without disabilities who
have access and functional needs.
State, tribal and local governments are responsible for maintaining plans to support emergency
response. Emergency managers and shelter planners should incorporate the planning considerations
addressed in this guidance into their existing plans.
16
Operational Tool #1 Planning Guidance
Comprehensive
Preparedness Guide 101
A Guide for All-Hazard
Emergency Operations
Planning
The FEMA Comprehensive Preparedness Guide, CPG 101
provides general guidelines on developing Emergency Operations
Plans (EOPs). It promotes a common understanding of the
fundamentals of planning and decision making to help emergency
planners examine a hazard and produce integrated, coordinated,
and synchronized plans. This guide helps emergency managers in
State, territorial, local, and tribal governments in their efforts to
develop and maintain a viable all-hazard EOP.
Source http://www.fema.gov/pdf/about/divisions/npd/CPG_101_V2.pdf
4.1.2. Stakeholder Coordination
All levels of government, working closely with the private sector, share the responsibility of
providing emergency shelter care to children and adults who need assistance. All citizens expect
their State and local governments to keep them informed and to provide assistance in the event of an
emergency or disaster.
In developing plans that will meet the needs of people requiring FNSS, emergency managers and
shelter planners should collaborate with all relevant stakeholders including:
• People requiring FNSS
• Agencies and organizations that provide FNSS
• Agencies and organizations that advocate for the rights of people requiring FNSS
• DME, CMS, PAS, and communication providers
Emergency managers and shelter planners can obtain assistance in identifying stakeholders by
accessing www.disability.gov.
The operational tools in this document are excerpts and examples taken from various agency and
jurisdictional documents throughout the United States. While they are not meant to dictate a State’s
policies or procedures, they do present ideas and practices that can be adapted to t each State’s
specic needs.
Operational Tool #2 Stakeholder Coordination
Sample State
Guidance to Address
Functional Needs
The New Hampshire Functional Needs Guidance includes the names
and contact information for direct service providers and advocacy
organizations that work with functional needs populations, such as faith-
based organizations, home-healthcare providers, Meals on Wheels, etc. In
addition, the document suggests that the State and local agencies that may
be of assistance include the: Developmental Disabilities Council, Area
Agencies, Governor’s Commission on Disability, Granite State Independent
Living, Northeast Deaf and Hard of Hearing Services, NH Association
for the Blind, NH Brain Injury Foundation, Community Action Programs,
Community Mental Health Centers and NH Ofce of Minority Health.
Source New Hampshire Functional Needs Guidance – Support Document to the
State Emergency Operations Plan
http://www.nh.gov/safety/divisions/hsem/stateemergplan/index.html
17
4.1.3. Planning Shelter Capacity
When anticipating and planning for shelter capacity, emergency managers and shelter planners
should:
• Be familiar with and committed to meeting ADA requirements for general population care
shelters
• Know the demographic prole of their community and understand the type of assistance that
may be required by various populations during an emergency or disaster
• Establish a rigorous public education program with an emphasis on personal preparedness.
(The program should include information in accessible formats and languages to reach the
entire community)
• Collaborate with stakeholders (see section above on Stakeholder Coordination)
• Ensure that emergency plans are a “living document” and are updated with a predetermined
frequency, as well as after any major event
• Establish mutual-aid agreements and memorandums of understanding with neighboring
communities that can provide additional emergency resources in the event that local shelters
are destroyed or damaged
Operational Tool #3 Planning Shelter Capacity
Sample of Available
Information Regarding
the Estimated Number of
Children and Adults in Texas
who have a Disability or
have Difculty Performing
Self-care Activities
In Texas, there are an estimated 2,962,000 people, age 5 and older,
who have a disability. Texas also has an estimated 579,000 people,
age 5 and older, who have difculty performing self-care activities.
This website presents the disability prevalence data by State or the
entire U.S. and is broken down by disability type, age, gender, race,
ethnicity, family income, benet recipiency, employment, and living
arrangement.
Source Center for Personal Assistance Services, University of California,
San Francisco, California
http://www.pascenter.org
Note: Click on Need for PAS, click on Disability Prevalence Data
from the Current Population Survey (2008-2009)
4.1.4. Identifying Shelter Sites/Facilities
Federal and State laws require that children and adults with disabilities have equal opportunity
to access emergency programs and services. An assumption might be made that if a building is
designated as a shelter, it will meet the needs of all individuals as long as it provides a safe place to
eat, sleep, and take care of personal hygiene needs. However, without modications, some shelters
are not appropriate to support the integration of FNSS. Emergency managers and shelter planners
should ensure that all general population shelters meet ADA requirements, including the standards for
accessible design and State accessibility codes.
Operational Tool #4 Locating the Shelter
Priority Site Selection Facilities that have been built or altered since 1992 are more likely to
comply with the architectural requirements of the ADA
Source ADA Best Practices Toolkit Chapter 7, ADA Checklist for
Emergency Shelters
www.ada.gov/pcatoolkit/chap7shelterchk.pdf
18
4.1.5. Evaluating the Shelter
Individuals who have the responsibility of selecting shelter sites are often not trained in what
constitutes an accessible facility. They need information to assist them in evaluating a building
to determine if it is accessible or can be made accessible expeditiously with few modications
and minimal expense. There are individuals in nearly every community who have experience in
evaluating accessibility (e.g., ADA Consultants, ADA accessibility inspectors, disability-related
organizations).
Preliminary analysis of each potential shelter will expedite the elimination of any building with
extensive barriers.
Operational Tool #5 Evaluating the Shelter-Site Selection Tool
ADA Checklist for
Emergency Shelters
Shelters need accessible:
• Entrances
• Routes to all services/activity areas
• Routes within toilet rooms
• Passenger drop off and pick up areas
• Parking
• Sidewalks and walkways
• Shelter entrances, hallways, and corridors
• Check in/information areas
• Sleeping areas
• Restrooms, showers, and toilet stalls, including portable toilets
• Public telephones
• Drinking fountains
• Eating areas
• Medical rst aid areas
• Recreation areas
The checklist provides instructions on taking measurements of the shelter.
Source www.ada.gov/pcatoolkit/chap7shelterchk.pdf; ADA Checklist for
Emergency Shelters; Appendix 1
4.1.6. Selecting the Shelter
State codes and standards must, at a minimum, meet the Federal requirements, but can be more
comprehensive. The ADA and other Federal laws, including the Stafford Act, the Rehabilitation
Act, the Fair Housing Act, and the Architectural Barriers Act, provide afrmative obligations
and prohibitions of discrimination on the basis of disability. No State or local government, or its
contractors, may, by law, policy, or contract, provide services below those standards without violating
Federal law. This does not mean that a State or local government cannot enact laws and ordinances
or provide services, obligations, and prohibitions that extend beyond these standards to ensure greater
access. A common example would be to provide twice as many as the required number of accessible
parking spaces and access aisles.
Since most States and communities have additional codes and standards related to accessibility,
emergency managers and shelter planners should be sure to identify and comply with these
requirements as well.
19
If selected as an emergency shelter, a facility with inaccessible features must be made accessible
before use as a shelter (reference Operational Tools #4 and #5 and Appendix 1).
Plans should include strategies to provide power for services that require a back-up power system in
an emergency or disaster. It is important to determine if a facility has a source of emergency power
generation.
Operational Tool #6 Florida Shelter Selection Checklist
Checklist for
Emergency
Shelters
Checklist for emergency shelters reecting Florida code
Source Americans with Disabilities Act/Florida Accessibility Code
Statewide Disability Coordinator
Telephone : 850-413-9892
http://www.oridadisaster.org/documents/ada/emergencyshelterchecklistorida.pdf
Operational Tool #7 San Jose California Shelter Assessment Checklist
Checklist for Assessing
Emergency Shelters
San Jose California tool for assessing an emergency shelter
Source San Jose Ofce of Emergency Services
http://www.sanjoseca.gov/emergencyservices
Note: Click on San Jose Disaster Shelter Annex for Vulnerable
Populations, click on Annex D
4.1.7. Equipping and Supplying the Shelter
Post-Katrina Emergency Management Reform Act (PKEMRA) requires that children and adults
with and without disabilities who have access and functional needs must be able to access the same
programs and services as the general population.
Despite best efforts and advance planning, some persons will arrive at the shelter without the durable
medical equipment (DME) and/or medications they require.
Prior to an emergency or disaster, emergency managers and shelter planners should:
• Include in the State plan a process for locating, purchasing, and storing as much of the supplies
and equipment as possible and practical to meet the needs of children and adults with and
without disabilities who have access and functional needs
• Develop provider agreements with the private sector to ensure that necessary equipment and
supplies that have not been purchased and stored will be available during an emergency or
disaster
• Develop agreements with area contractors to maintain equipment (e.g., generators, oxygen
concentrators)
20
Emergency managers and shelter planners should include in the planning process people with
expertise and experience in dealing with the logistical requirements of providing the resources
necessary to set up and operate a general population shelter that includes children and adults with and
without disabilities who have access or functional needs.
Operational Tool #8 Durable Medical Equipment (DME) List
DME (for children and adults) Sample DME list
Source FEMA: Durable Medical Supply Sample List; Appendix 3
Operational Tool #9 Consumable Medical Supplies (CMS) List
CMS (for children
and adults)
Sample list of Consumable Medical Supplies using a planning estimate
based on 100 person shelter population for one week
Source FEMA: Consumable Medical Supply Sample List; Appendix 4
Operational Tool #10 Communication Devices
Communication Devices
(not inclusive)
• Hearing aids
• TTY/TDD Phones
• Cap Tel Phones (for captioning)
• Computer Assisted Real time Translation
• Hearing aid batteries of different sizes (including batteries for
cochlear implants
• Synthesizers used with PCs for text-to-speech
• Screen Readers
• Screen Magnication Programs
• Scanning Systems for Low Vision Users
Source Guidance on Planning and Responding to the Needs of People with
Access and Functional Needs, California Emergency Management
Agency, Ofce for Access and Functional Needs
www.oes.ca.gov/
Click on Ofce for Access and Functional Needs
Source BCFS; www.bcfs.net/fnssrecommendations
Operational Tool #11 Resources for Assistive Technology
Reuse of Assistive
Technology
There is at least one Federally-funded program in every State that engages
in the reuse of assistive technology. These programs are also connected to
other entities in the State that reuse assistive technology so they can serve as a
central point of contact for emergency managers and shelter planners.
Source http://www.resnaprojects.org/nattap/at/statecontacts.html
(contact information only)
Source http://www.resnaprojects.org/nattap/at/statecontacts.html#al
(contact information)
21
Operational Tool #12 Legal Authority-DME, CMS, Communication Devices
Legal Authority
Federal agencies may, on the direction of the President, provide assistance
essential to meeting immediate threats to life and property resulting from a
major disaster including:
• Medicine, durable medical equipment, communication devices, goods,
and other consumables
• Emergency medical care, emergency mass care emergency shelter, and
provision of food, water, medicine, durable medical equipment
In any emergency, the President may:
• Assist State and local governments in the distribution of medicine, food,
and other consumable supplies, and emergency assistance
Federal authority for provision of PAS can be found in the reference below.
Source Sections 403 (a) (2) and (3) (B) and 502(a) (7) of the Robert T. Stafford
Disaster Relief and Emergency Assistance Act, 42 U.S.C. §§ 5121-5206, as
amended. Federal Disaster Assistance, 44 C.F.R. pt. 206.
http://www.fema.gov/about/stafact.shtm
Many children and adults with and without disabilities who have access and functional needs depend
on battery-powered wheelchairs and scooters for mobility. The batteries in these mobility aids must
be recharged frequently or they will stop functioning. Without these mobility aids, individuals will
lose their ability to move about, they may be unable to participate in some services offered by the
shelter, and they may need to depend more heavily on assistance from caregivers.
4.1.8. Locating Services
State plans should include arrangements for services that are necessary to provide sufciency of
care in order to maintain level of function for children and adults with and without disabilities who
have access and functional needs in a general population shelter. Emergency managers and shelter
planners should arrange for services ahead of time through the use of provider agreements. The
following are examples of some types of services that should be available in a general population
shelter:
• Power Generation
◦ Redundant source of power even in the event of a long-term power outage. Some facilities
may have no source of emergency power generation, while others may have only a
limited source. Emergency managers and shelter planners should take whatever steps are
necessary to see that there is a plan for providing an alternate source of power in the event
of an outage and mechanical service contracts/services for emergency repairs.
• Medical Providers
◦ Physicians, Registered Nurses, Licensed Vocational Nurse, EMT’s and Paramedics
◦ Psychiatrists and Dental providers
◦ Emergency veterinary service provider
◦ Access to dialysis treatments (this includes providing access to transportation to and from
the dialysis facility and a meal(s) if a resident is not at the shelter during meal time(s))
• Communications providers
◦ Interpreters (Spanish, sign language, etc.)
◦ Television with captioning
◦ Information technology/computer services
◦ TTY - TDD
22
◦ Computer Assisted Real time Translation (CART)
◦ Note taking
• Food service providers
◦ Special diets
◦ Caterer
• Transportation providers
◦ Para transit services
◦ Public transportation
• Shelter Maintenance providers
◦ Service for accessible portable toilets, hand washing units, showers, etc.
◦ Disposal of bio-hazard materials, such as needles in sharps containers
• DME providers
◦ Oxygen providers
• CMS providers
Operational Tool #13 Locating Services
Support
Services
Staff and resources to:
• Replace prescribed medications
• Obtain DME and CMS
• Assist persons in maintaining their usual level of independence (personal
assistance with activities of daily living, older adult non-acute medical and
chronic conditions, etc.)
• Provide support to persons with intellectual, cognitive, and mental health
conditions
• Provide interpreters and/or other communication support to assist persons who
require communication assistance deaf or hard of hearing and blind or low
vision, speech disabilities, language/cultural differences
• Provide assistance to individuals who have conditions that affect mobility
• Provide assistance to children and adults with chronic but stable respiratory
conditions (heart disease, asthma, emphysema, allergies, etc.)
• Provide assistance to children and adults with temporary limitations (post-
surgery, injuries, pregnancy, etc.)
• Provide assistance to children and adults who require dialysis
Source Guidance on Planning and Responding to the Needs of People with Access and
Functional Needs, California Emergency Management Agency, Ofce for Access and
Functional Needs
www.oes.ca.gov/
Note: Click on Ofce for Access and Functional Needs
Source BCFS; www.bcfs.net/fnssrecommendations

23
Operational Tool #14 Documenting Service Providers
Service Provider
Contact Information
Form used to document names, vendor number, addresses and telephone
numbers of service providers including:
Communications Providers
• Interpreters (Spanish, sign language, etc.)
• Television with captioning
• Information Technology/Computer Services
• TTY-TDD
• Computer Assisted Real time Translation (CART)
• Note taking
Medical Stafng Services
• On-site nursing services
• Emergency medical services
• Emergency dental services
• Pharmaceutical services
Resource Suppliers
• O2
• Dialysis
• Constant power source
• Blood sugar monitoring
Food Services
• Special diets
• Caterer
Personal Assistance Services
Transportation Services
• Para transit Services
• Public Transportation
Service Animals
• Emergency veterinary services
Shelter Maintenance Services
• Servicing of accessible portable toilets, hand washing units, etc.
• Disposal of bio-hazard materials
FNSS equipment
• Durable Medical Equipment
Source BCFS; www.bcfs.net/fnssrecommendations; FORM: Contact Information
for Shelter Services Providers; Appendix 2
4.1.9. Stafng the Shelter
Emergency managers and shelter planners should integrate people with expertise regarding access and
functional support needs into the stafng plan. Agencies in the stakeholder group are often a good
resource for providing shelter staff with appropriate experience (reference section on Stakeholder
Coordination).
Operational Tool #15 Stafng the Shelter
Personal Assistance
Services
Guidance for providing personal assistance service in general population
shelters that include children and adults with access or functional needs
Source BCFS; www.bcfs.net/fnssrecommendations in conjunction with FEMA;
www.fema.gov; Guidance on Providing Personal Assistance Services;
Appendix 5
24
4.1.10. Assessment Teams
Prior to a disaster or emergency, there should be a plan for the activation of a shelter assessment team
to assess the needs of children and adults who have access or functional needs. An entity may want
to develop a process to credential these teams. One example of a team is the California Functional
Assessment Service Team (FAST) described below. The FAST training is a DHS-approved course.
Operational Tool #16 Assessment Teams
Functional
Assessment
Service Team
(FAST)
The FAST responds to the needs of people in a shelter who have access or
functional needs. The purpose of the FAST program is to conduct assessments
of people with these needs as they arrive at the general population shelters. The
assessment evaluates the functional needs a person has and determines resources
necessary to support these needs in the general population shelter.
The FAST may be deployed as shelters are opened and remain in service until
they are no longer needed. They can also transfer to another shelter as needed,
or request to deploy to shelters as jurisdictions become aware of their existence
during major events.
FAST consists of trained government employees and personnel from community-
based organizations and non-governmental organizations ready to respond and
deploy to disaster areas to work in shelters. The FAST members should have
extensive knowledge of the populations they serve, their needs and available
services and resources including housing, benet programs and disaster aid
programs. They assist in meeting essential FNSS so people can maintain their
usual level of independence during disasters and emergencies. FAST frees
up other emergency resources to focus on emergency incidents rather than on
mitigating complications.
FAST planning includes:
• Training teams
• Establishing a Memorandum of Understanding with individuals or
organizations that will participate in the FAST
• Maintaining contacts at the State, tribal, regional, and local level
Source Guidance on Planning and Responding to the Needs of People with Access and
Functional Needs, California Emergency Management Agency, Ofce for Access
and Functional Needs
www.oes.ca.gov/
Note: Click on Ofce for Access and Functional Needs
DHS approved FAST course (CA-049-REST)
http://www.dss.cahwnet.gov/dis/PG1909.htm
Homeland Security Grant Program and Emergency Management Program Grant
funds can be used to implement this program (California Department of Social
Services).
25
4.1.11. Shelter Layout
Cots and other furniture items are placed in such a way that routes are accessible to people who use
wheelchairs, crutches, or walkers. Protruding objects in ANY area where people walk throughout
the shelter should be eliminated. Accessible routes should connect the sleeping quarters to the food
distribution and dining quarters, bathrooms, and activity areas (reference Chapter 7 Addendum 2:
The ADA and Emergency Shelters: Access for All in Emergencies and Disasters).
Operational Tool #17 Shelter Layout
Estimating Shelter
Capacity
• 20 square feet per person should be available for short-term
or evacuation shelters and up to 40 square feet per person for
sheltering longer than 72 hours
• People who use wheelchairs, lift equipment, a service animal, and
personal assistance services can require up to 100 square feet
Source Sheltering People with Disabilities, Draft Space and Layout
Considerations Universal Access Committee, Feb, 2007
www.ct.gov/demhs/lib/demhs/space__layout_considerations.pdf
4.1.12. Shelter Intake
Individuals are not required to provide information about their disability or access or functional
needs, but the opportunity to provide that information must be given. Emergency managers and
shelter planners should include in their plans specic strategies for complying with the legal mandate
that people with disabilities must be able to access the same programs and services as the general
population. An individual request for an accommodation, based on disability, should be provided
even if not requested during the initial intake.
26
27
4.2. Key Considerations
In Planning For Shelter
Operations
Segregating children and adults with and without disabilities who have access or functional needs and
those with whom they are associated from general population shelters to “special needs” shelters is
ineffective in achieving equitable program access and violates Federal law. People with disabilities
are entitled by law to equal opportunity to participate in programs, services, and activities in the most
integrated setting appropriate to the needs of the individual. Additionally, children and adults with
and without disabilities who have access and functional needs should not be sheltered separately from
their families, friends, and/or caregivers because services they require are not available to them in
general population shelters.
28
4.2.1. Dietary
Plans should include provisions to ensure meals and snacks are provided to all shelter residents,
including children and adults with specic dietary needs and restrictions (e.g., people with diabetes
or severe allergies to common food ingredients and baby formulas). Plans should also include a
process for responding quickly to unanticipated, but legitimate, dietary needs and restrictions that are
identied when a resident is admitted to the shelter. It is critical that information about any special
dietary needs or restrictions be obtained, documented, and communicated to the entity responsible for
meal and snack preparation immediately. Food preparation may need to be adjusted (e.g., food may
need to be pureed) to meet resident needs.
Operational Tool #18 Dietary-Agreement
Resources
for Meeting
Dietary Needs
Develop a memorandum of agreement or contract with a local organization(s)
that has demonstrated capacity to provide meals and snacks to large populations
including:
• Hospitals
• Local restaurants or cafeterias
• Schools
• Non-prots with a feeding crew
Source BCFS; www.bcfs.net/fnssrecommendations
Source Multi Agency Feeding Plan; http://www.nvoad.org/index.php/rl/doc_download/8-
multi-agency-feeding-plan.html
In order to meet all the needs of all people in the shelter, menus that are low sodium, low fat and low
sugar should be developed for general population shelters and should include specic instructions
regarding what to purchase in order to prepare each meal. Organizations contracting to prepare meals
and snacks should also anticipate and be prepared to provide meals for persons with other dietary
restrictions (e.g., vegetarian, gluten-free meals, kosher meals, meals for people who are allergic to
peanut oil and by-products).
Operational Tool #19 Dietary-Menu
One Day Menu for General
Population Shelter
Menu for general population shelters, including modications for
persons who are diabetic, require reduced sodium, pureed diets and
infants and children
Source BCFS; www.bcfs.net/fnssrecommendations; One Day Menu for
General Population Shelters Providing Functional Needs Support
Services; Appendix 6
4.2.2. Service Animals
Under the ADA, a service animal is any animal that is individually trained to provide assistance to a
person with a disability. Most people are familiar with dogs that guide people who are blind or have
low vision, but there are many other functions that service animals perform for people with a variety
of disabilities. Examples include alerting people who are deaf or hard of hearing to sounds; pulling
wheelchairs; carrying or retrieving items for people with mobility disabilities or limited use of arms
or hands; assisting people with disabilities to maintain their balance or stability; alerting people to,
and protecting them during, medical events such as seizures; and working or performing tasks for

29
individuals with psychiatric, neurologic, or intellectual disabilities, such as waking up a person with
depression, assisting a person with Alzheimer’s in way-nding, retrieving misplaced objects for
persons with traumatic brain injury, protecting a child with autism from self injury, or orienting an
individual with schizophrenia to their environment.
Many emergency shelters do not allow residents or volunteers to bring their pets or other animals
inside, but shelters must make exceptions to “no pets” or “no animals” policies to allow people with
disabilities to be accompanied by their service animals. Service animals are not pets and are therefore
not subject to restrictions applied to pets or other animals.
While dogs are the most common type of service animal, other types of animals can also be service
animals. There are also no limitations on the size or breed of dogs that can be used as service animals.
Many service animals are easily identied because they wear special harnesses, capes, vests, scarves,
or patches. Others can be identied because they accompany individuals with visible disabilities and
the functions they perform can also be readily observed. When none of these identiers are present,
shelter staff may ask only two questions to determine if an animal is a service animal:
(1) “Is this a service animal required because of a disability?”
(2) “What work or tasks has the animal been trained to perform?”
If the answers to these questions reveal that the animal has been trained to work or perform tasks
or services for a person with a disability, it qualies as a service animal and must be allowed to
accompany its owner anywhere other members of the public are allowed to go, including bathrooms,
areas where food is served, and almost all areas where medical care is provided. Questions about the
nature or severity of a person’s disability or ability to function may not be asked. The ADA also does
not permit shelter staff to question a person’s need for a service animal or exclude a service animal
on the grounds that shelter staff or volunteers can provide the assistance normally provided by the
service animal. Under the ADA, shelter staff may not require a license, certication, ID tag, medical
certicate, or any other type of documentation for a service animal.
Operational Tool #20 Service Animals Denition
ADA Best Practices Tool
Kit, Chapter 7 Addendum 1
The ADA and Emergency Shelters: Access for All in Emergencies
and Disasters, pages 6-7
Source http://www.ada.gov/pcatoolkit/chap7shelterprog.pdf
In addition to the requirements set out in the ADA, the shelter may be covered by the Fair Housing
Act (FHA). The FHA affords individuals with disabilities the right to use service animals in housing.
Plans should direct that, prior to an emergency or disaster, the following issues be addressed:
• Areas where animals can be housed, exercised, and toileted should be identied and
communicated in alternative accessible formats in each general population shelter
• A reliable source for food and supplies (water bowls, leashes, collars) for the animals should
be located and agreements be made to ensure that these items are available
30
4.2.3. Communication
Effective communication is essential during an emergency or disaster. Children and adults with
and without disabilities who have access or functional needs should be given the same information
provided to the general population using methods that are understandable and timely. The ADA
states that a public entity shall take appropriate steps to ensure that communication with applicants,
participants, and members of the public with disabilities are as effective as communication with
others. Effective communication requirements also apply to private and non-prot entities providing
sheltering services.
Plans should direct that, prior to an emergency or disaster, the auxiliary aids and services necessary to
meet the communication needs of all persons in the shelter are identied and immediately available.
Where possible, emergency managers and shelter planners should already have contracts and/or
memorandums of agreement in place with the vendors who can provide these items and services.
Operational Tool #21 Communication-Strategies
General Assign volunteers ahead of time to provide one-on-one assistance
to residents who need help in providing and receiving effective
communication throughout the sheltering process (e.g., completing forms)
Blind and Low Vision Provide Braille, large and high contrast print, audio recording, readers
Deaf or Hard of
Hearing, Speech
Disability
Provide qualied sign language or oral interpreter; augmentative
communication device; post message in central location; have notepads,
pens and pencils
Intellectual Disability Present information slowly, use simple language and speak in short
sentences
Source FEMA: Accommodating Individuals with Disabilities in the Provision of
Disaster Mass Care, Housing and Human Services
http://www.fema.gov/oer/reference/index.shtm
Source Chapter 7 Addendum 2: The ADA and Emergency Shelters: Access for
All in Emergencies and Disasters
http://www.ada.gov/pcatoolkit/chap7shelterprog.pdf
Operational Tool #22 Communication-Devices
Communication
Devices
All communication devices must be accessible to people with access or
functional needs
Telephone Access to teletypewriter (TTY or TDD or CapTel)
Television Accessible captioning
Computers Equipment and programs that make computers accessible to people who
are deaf, blind, those who have intellectual or mobility disabilities
Source BCFS; www.bcfs.net/fnssrecommendations
In each case, the type of auxiliary aid or service required depends on several factors, including
the length, complexity and importance of the communication and the person’s language skills
and history. For example, it is no help to have an American Sign Language (ASL) interpreter
available to communicate with deaf residents if the resident uses Signed English or other forms of
communication.
31
4.2.4. Bathing and Toileting Needs
Whenever bathing and toileting facilities are available in a general population shelter they must
include accessible bathing and toileting facilities for children and adults. If a shelter does not have
accessible facilities or if there are very limited accessible facilities available, plans should include
ways this limitation will be addressed. This can include agreements with private contractors to
provide these facilities.
Operational Tool #23 Bathing and Toileting Ratios – Red Cross
Portable Accessible Showers,
Toilets, and Sinks
Red Cross ratio: The American Red Cross recommends that, on
average, there should be one toilet for every 20 persons in the
shelter. Count only those facilities that will be accessible to shelter
residents and shelter staff.
Source American Red Cross Mass Care Standards and Indicators,
Version 011-072209
Many emergency managers and shelter planners look for specic ratios regarding the number of toilet
rooms, showers, and baths to provide at an emergency shelter. In the context of the ADA Standards,
the obligation will depend on what type of toilet facility is provided (e.g., a single-user toilet room, a
toilet room with stalls).
Generally, each toilet room with stalls must have at least one fully accessible, standards-compliant
water closet/stall (see 28 C.F.R. pt. 36, App. A, ADA Standards for Accessible Design §§ 4.1.2(6),
4.16, 4.17, 4.18, 4.19, 4.22, Figs. 29, 30, 31, and 32). This includes appropriate side and rear
grab bars, sufcient clear oor space, the toilet seat must be between 17-19 inches from the
nished oor, and the centerline of the toilet must be 18 inches from the side wall, among several
other requirements. For further explanation and a tool to determine adequacy to meet the ADA’s
requirements, see ADA Best Practices Toolkit, Chapter 7 Addendum 3: ADA Checklist for Emergency
Shelters: www.ada.gov/pcatoolkit/chap7shelterchk.htm.
If there are six or more water closets/stalls in a toilet room, then one of the stalls, in addition to the
accessible stall, must be an ambulatory stall with parallel grab bars and an outward swinging door
(see 28 C.F.R. pt. 36, App. A, ADA Standards for Accessible Design §§ 4.22.4, 4.26, and Fig. 30(d)).
When portable toilet units are clustered together at emergency shelters, at least 5% of each cluster
must be accessible portable toilet units, identied by the International Symbol of Accessibility (see 28
C.F.R. pt. 36, App. A, ADA Standards for Accessible Design § 4.1.2(6)).
Standards also exist for the provision of baths and showers when provided. None of these
requirements prohibit, and emergency managers are encouraged to include, more accessible facilities
than required or mandated by Federal law, so long as they are otherwise standards-compliant.
32
4.2.5. Quiet Area
Plans should include a strategy for providing a quiet area within each general population shelter. The
stress that is created during and after an emergency or disaster is increased as a result of the noise and
crowded conditions of a shelter. Without access to a quiet room or space, some people (e.g., elderly
persons, people with psychiatric disabilities and parents with very young children, children and adults
with autism) will be unable to function in a shelter environment (see Chapter 7 Addendum 2: The
ADA and Emergency Shelters: Access for All in Emergencies and Disasters: http://www.ada.gov/
pcatoolkit/chap7shelterprog.pdf ).
4.2.6. Mental Health Services
Because there are differences in State and local laws, rules and regulations related to the provision of
mental health services, it is important that, early in the planning process, emergency managers and
shelter planners seek guidance from people with disabilities and others with access and functional
needs and appropriate State and local authorities regarding these matters.
Emergency managers and shelter planners should include people with expertise regarding children
and adults with and without disabilities who have access and functional needs in the mental health
stafng plan. Agencies in the stakeholder group are often a good resource for shelter staff with
appropriate experience (reference section on Stakeholder Coordination).
Ideally, plans should include a directive to pre-identify a licensed mental health professional(s) who
will be present in a general population shelter at all times. If that is not possible due to a lack of
resources, then plans should provide that a licensed mental health professional is on call to a shelter at
all times. Where possible, a psychiatrist should also be on call at all times.
Operational Tool #24 Mental Health Services
Sources for
Mental Health
Services
Sources include colleges and universities (faculty and students), mental health
organizations, social services agencies, and places of worship.
The New Jersey Division of Mental Health Services (DMHS) within the New
Jersey Department of Human Services (NJDHS) has over 120 contracted
community mental health provider agencies.
Substance Abuse and Mental Health Services Administration (SAMHSA) has
the contract to provide mental health counseling in emergency situations.
Source BCFS; www.bcfs.net/fnssrecommendations
Source http://www.samhsa.gov/dtac/
4.2.7. Medical and Dental Services
Because there are differences in State and local laws, rules, and regulations related to the provision of
medical and dental care, it is important that, early in the planning process, emergency managers and
shelter planners seek guidance from appropriate State and local authorities regarding these matters.
33
Children and adults with and without disabilities who have access or functional needs who require
medical services may not be excluded from a general population shelter. Plans should direct that,
at a minimum, medical care that can be provided in the home setting (e.g., assistance in wound
management, bowel or bladder management, or the administration of medications or use of medical
equipment) is available to each general population shelter.
Plans should be in place for addressing medical and dental care decisions at all times. This could
include making contracts/agreements prior to an emergency or disaster for the personnel and
supplies necessary to set up and staff a rst aid station at each shelter site. Having these plans in
place is intended to prevent inappropriate transfers to medical facilities. This will benet the whole
community by maximizing resources and limiting medical surge.
A comprehensive list of emergency medical and dental services in the area should be maintained at all
times.
Operational Tool #25 Medical Station
Onsite Medical Staff • Provide OTCs
• Implement methods to minimize contagion
• Make referrals for emergency medical and dental treatment
Medical Station Staff with a minimum of 1 RN and 1 paramedic at ratio of 1:100 shelter
residents at all times
Oncall Medical Staff Maintain on call physician and psychiatrist 24/7
Source BCFS; www.bcfs.net/fnssrecommendations
Operational Tool #26 Disaster Health Response and Care
Services • Perform health assessments and referrals
• Implement infection control methods and perform illness and injury
surveillance
• Facilitate replacement of medications, CMS and DME
Shelter Stafng Staff with 1 licensed health professional (minimum licensure is EMT) at
ratio of 1:100 shelter residents at all times
Source American Red Cross; www.redcross.org
Plans should also include a requirement to document any medical care provided at the shelter and a
strategy for accomplishing these efforts.
Operational Tool #27 Medical Services-Form
Resident Health Care
Record
Form to document a resident’s visit to the rst aid station and any off-
premises medical or dental care
Source BCFS; www.bcfs.net/fnssrecommendations; FORM: Resident Health Care
Information; Appendix 7
In the event of a medical or dental emergency, plans should direct shelter staff to call 911 and refer
residents for medical or dental care, as appropriate.
34
4.2.8. Medication
Because there are differences in State and local laws, rules, and regulations related to the storage,
preparation, administration, documentation, and disposal of medications, it is important that, early in
the planning process, emergency managers and shelter planners seek guidance from appropriate State
and local authorities regarding these matters.
The fact that a person has or requires medications is not a basis for excluding him/her from a general
population shelter. Plans should include procedures for obtaining, storing, dispensing, documenting,
and disposing of medications in a general population shelter.
Plans should ensure that shelter residents have access to medications. One way to accomplish this is
to have contracts or agreements in place with a pharmacy(s) to make medications available to shelter
residents. This will minimize the time a resident has to go without necessary medications.
Operational Tool #28 Medication
Filling Prescriptions When a pharmacy(s) is part of a chain of pharmacies, the pharmacist may
be able to obtain information about a shelter resident’s medications by
checking records kept in a centralized location away from the community
where the emergency or disaster occurred.
Storage As a rule, residents are responsible for safeguarding, storing, and
administering their own medication. If that is not practical (due to need for
refrigeration, concerns regarding drug security, or the ability of the resident
to self-medicate), residents’ prescription medications should be kept in a
locked container used exclusively for that purpose at the rst aid station.
Disposal If medications are kept in the rst aid station, staff should return all
resident medications, including those that have been discontinued or have
passed the expiration date, when the resident is discharged from the shelter.
Needles or hypodermic syringes with needles attached must be disposed of
in bio-hazard containers.
Source BCFS; www.bcfs.net/fnssrecommendations; FORM: Medication
Administration Record; Appendix 8
Operational Tool #29 Medication-Emergency Prescription Assistance Program (EPAP)
Program Description EPAP, a joint program of FEMA and the Department of Health and
Human Services, provides an efcient way for pharmacies to process
claims for prescription medications and limited DME for individuals
who have no insurance coverage and are from an area declared as
a disaster by the President. Claims for individuals with private
insurance, employer-sponsored coverage, public insurance, or other
third party coverage are not eligible for payment under the EPAP.
Services Provided Provides a 30-day supply of essential pharmaceutical and DME lost as
a direct result of the disaster or as a secondary result of loss or damage
caused while in transit from the emergency site to the designated
shelter facility.
Participating Pharmacies Any enrolled pharmacy in the U.S. and its territories
Source http://www.hhs.gov/aspr/opeo/epap/index.html
35
Sections 403 (a) (2) and (3) (B) and 502(a) (7) of the Robert T. Stafford Disaster Relief and
Emergency Assistance Act, 42 U.S.C. §§ 5121-5206, as amended. Federal Disaster Assistance, 44
C.F.R. pt. 206.
http://www.fema.gov/about/stafact.shtm
4.2.9. Transportation Services
Children and adults with and without disabilities who have access or functional needs may require
transportation services while in shelters and for re-entry into the community. Emergency managers
and shelter planners should see that plans include strategies to ensure that accessible vehicles,
ambulances, and drivers are available to the shelter.
Accessible vehicles should be able to transport wheelchairs, scooters, or other mobility aids, as well
as equipment and supplies (e.g., portable oxygen, portable toilets, communication devices, service
animals). Even if accessible public or private transportation is ordinarily available, there should be a
contingency plan for transporting people if this transportation is disrupted.
Contingency plans for hazards occurring during a sheltering event should include readily available
resources for transporting people with access and functional needs, as well as their life sustaining
equipment, to alternative shelter sites.
Operational Tool #30 Transportation Services
Transportation Accessible
Resources
Potential accessible resources include:
• Local school districts with lift-equipped school buses
• Community EMS services
• Vans from places of worship
• Local assisted living facility vans
• Local community and public transit vehicles
• Para transit services
• Dial-a-Ride
• Fixed route buses
• Area agencies on aging
• Regional center vendors
• Taxi systems
• Non-medical emergency services
• Adult day health care vehicles
• Airport car rental shuttle buses
• Airport shuttle buses
• Older adults center vendors
• Health care center vendors
Source Guidance on Planning and Responding to the Needs of People with
Access and Functional Needs, California Emergency Management
Agency, Ofce for Access and Functional Needs
www.oes.ca.gov/
Click on Ofce for Access and Functional Needs
Source
BCFS; www.bcfs.net/fnssrecommendations

36
Plans should include:
• An agreement or contract with transit providers in place prior to an emergency or disaster
• A pre-determined process for reimbursing transit providers for their services
Note that transportation providers may have prearranged agreements with multiple entities that would
result in insufcient services if an emergency affected an entire State or region.
Operational Tool #31 Transportation Services - Form
Transportation Request Form to request resident transportation for:
• Appointments and activities while living at the shelter
• Returning home or to temporary house at discharge
Source BCFS; www.bcfs.net/fnssrecommendations; FORM: Transportation
Request Information; Appendix 9
37
4.3. Key Considerations In
Planning For Transition/
Recovery
4.3.1. Transitioning Back to the Community
In order for children and adults who have access or functional needs to transition back to their
community, it is important to provide them a reasonable amount of time and assistance to locate
suitable housing when they cannot return to their former homes. In the past, shelters have sometimes
required people needing FNSS to move to hospitals, nursing homes, or other institutions because
they could not quickly locate suitable housing or the supportive services needed to live on their
own. As a result, people who once lived independently in their own homes have found themselves
institutionalized soon after an emergency or disaster occurred.
To comply with ADA requirements and assist people in avoiding unnecessary institutionalization,
emergency managers and shelter planners should include strategies for children and adults with
functional support needs in their plans to have the time and assistance required to:
• Return to their homes, or
• Locate new homes in the most integrated setting that is appropriate to their needs
Organizations providing direct services to people with disabilities and others with access or functional
needs should be included in all local assistance and disaster recovery efforts to:
• Promote coordination with one other
• Maximize resources
• Eliminate duplication
Operational Tool #32 Transitioning Back to the Community
Gap Analysis Tool for:
• Re-entry
• Demobilization
• Trigger point established for when to return children and adults
• Transport plan for individuals unable to get home from
transportation assembly points
• Trigger points established for when to demobilize transit resources
• Procedure established to check-out emergency evacuation
resources
• Procedure established to debrief demobilizing personnel
• Procedure established to debrief children and adults
• Demobilization procedures reviewed at least annually
Source Guidance on Planning and Responding to the Needs of People with
Access and Functional Needs, California Emergency Management
Agency, Ofce for Access and Functional Needs; www.oes.ca.gov/
Note: Click on Ofce for Access and Functional Needs
Every effort should be made to move residents back to the least restrictive environment.
38
Operational Tool #33 Transitioning Back to the Community - Recovery
Possible Recovery
Needs
• Short- and long-term housing and wrap-around housing
(Accessible)
• Communication
• Replacement of DME and assistive technology
• Personal assistance services
• Transportation
• Financial assistance
Source Guidance on Planning and Responding to the Needs of People with
Access and Functional Needs, California Emergency Management
Agency; www.oes.ca.gov/
Note: Click on Ofce for Access and Functional Needs
Operational Tool #34 Transitioning Back to the Community - Re-entry
Re-entry Planning
Strategy
Prior to an emergency/disaster:
• Locate and document all available accessible hotel/motel rooms in
the community
• Develop contracts/agreements with these entities to reserve
resources for people with access or functional needs
• Determine a process for reimbursing businesses for these resources
Source BCFS; www.bcfs.net/fnssrecommendations
4.3.2. Closing the Shelter
It is important to remember that shelters are temporary and every effort should be made to close the
shelter by identifying and using the resources necessary to return residents to suitable housing that
continues to meet their access and functional needs. The goal is to always support individuals toward
self sufciency.
Operational Tool #35 Closing the Shelter
Considerations when
Closing a Shelter
Consider:
• Impact of the emergency or disaster on the home or environment of
a person with access or functional needs (e.g., a person’s home is not
damaged but rest of the neighborhood is gone, power out, etc.)
• The urgency of the need to return the shelter to normal conditions
• Availability of accessible transportation resources
Source Kansas Statewide Emergency Management; http://www.srskansas.org/
Note: Click on SRS Statewide Emergency Management, click on Assisting
Individuals with Functional Needs During Evacuation and Sheltering, scroll
down to Functional Needs Shelter Deactivation
Recovery is typically the longest and most difcult part of an emergency or disaster for all residents
of a community. It is further complicated when people with disabilities and others with access
or functional needs do not have access to personal assistance services, service animals, friends,
neighbors, neighborhood businesses and even family members.
39
Operational Tool #36 Closing the Shelter- Discharging Residents
Considerations when
Discharging a Resident
Requiring FNSS
Form documenting a resident’s discharge from the facility including
conrmation that a resident is discharged to his/her home:
• Determined by police or other emergency management personnel
in his or her community that he/she can return
• Contacted his or her landlord or neighbor to determine whether his
or her house is habitable
• Conrmed that any prior in-home services are restored (e.g.,
Meals on Wheels, Mental Heath Authority, Personal Assistance
Services)
• Conrmed access to businesses necessary to return home (e.g.,
grocery store, pharmacy
Source BCFS; www.bcfs.net/fnssrecommendations; FORM: Resident Discharge
Information; Appendix 10
Emergency managers and shelter planners can do little to counter some of the conditions people with
FNSS face during the recovery phase. They can, however, develop strategies so that the most critical
services and functional needs are restored or addressed as a priority during this phase.
Operational Tool #37 Closing the Shelter- Recovery
Recovery Plan
Considerations
• Making allowances at blockades, shelters, and other impacted
areas for access to people providing personal assistance services,
home health aids, visiting nurses, interpreters, support or service
animals, and other individuals crucial to immediate functional
needs of individuals
• Identifying the impact an interruption in utility services would
have on children and adults with and without disabilities who have
access and functional needs
• Planning for accessible shelter and appropriate temporary housing
needs
• Addressing how people with disabilities and others with access or
functional needs who are employed by businesses that are able to
open soon after a disaster will get to work
• Involving representatives of the functional needs community in
“after action reviews” or “hot wash reports” in order to capture the
true impact of the disaster and to improve plans for the future
Source New Hampshire Functional Needs Guidance – Support Document to the
State Emergency Operations Plan http://www.nh.gov/safety/divisions/
hsem/stateemergplan/index.html
Ideally, emergency managers and shelter planners should include the infrastructure needed to support
recovery in the State plan long before an emergency or disaster occurs.
40
5. Acronyms
ADA Americans with Disabilities Act
AED Automated External Debrillator
ASL American Sign Language
CART Computer Assisted Real time Translations
CBO Community-Based Organization
CDC Centers for Disease Control and Prevention
CMS Consumable Medical Supplies
DME Durable Medical Equipment
DRA Disability Related Assistance
EPAP Emergency Prescription Assistance Program
FAST Functional Assessment Service Teams
FEMA Federal Emergency Management Agency
FNSS Functional Needs Support Services
ICP Incident Command Post
IMT Incident Management Team
OTC Over-the-counter Drugs
PAS Personal Assistance Services
SOP Standard Operating Procedures
TDD Telecommunications Device for the Deaf
TTY Teletypewriter
VOAD Voluntary Organizations Active in Disasters
41
6. Glossary
Access
The ability to fully use, enjoy, and integrate into any programs, services, activities, goods,
facilities, privileges, advantages, or accommodations provided by a public or private (for-prot or
not-for-prot) entity, any contracted entity, or entity that provides emergency services, including
sheltering, for individuals with disabilities as dened by the ADA Amendments Act of 2008, P.L.
110-325, and those associated entities. Access may include modications to programs, policies,
procedures, architecture, equipment, services, supplies, and communication methods.
Access and Functional Needs
Those actions, services, accommodations, and programmatic, architectural, and communication
modications that a covered entity must undertake or provide to afford individuals with
disabilities a full and equal opportunity to use and enjoy programs, services, activities, goods,
facilities, privileges, advantages, and accommodations in the most integrated setting, in light
of the exigent circumstances of the emergency and the legal obligation to undertake advance
planning and prepare to meet the disability-related needs of individuals who have disabilities as
dened by the ADA Amendments Act of 2008, P.L. 110-325, and those associated with them.
Access and functional needs may include modications to programs, policies, procedures,
architecture, equipment, services, supplies, and communication methods. Examples of “access
and functional needs” services may include a reasonable modication of a policy, practice, or
procedure or the provision of auxiliary aids and services to achieve effective communication,
such as: (1) an exception for service animals in an emergency shelter where there is a no pets
policy; (2) the provision of way-nding assistance to someone who is blind to orient to new
surroundings; (3) the provision of transferring and toileting assistance to an individual with a
mobility disability; and (4) the provision of an interpreter to someone who is deaf and seeks to ll
out paperwork for public benets.
Action Plan
A plan developed by a case manager and resident(s) to assist and support that individual or family
in obtaining transitional or permanent living arrangements.
Cap Tel
A communication system that provides written captions of everything a caller says on a built-in
display.
Consumable Medical Supplies (CMS)
Medical supplies (medications, diapers, bandages, etc.) that are ingested, injected, or applied and/
or are one time use only.
42
Disability
The term “disability” has the same meaning as that used in the ADA Amendments Act of 2008,
P.L. 110-325, as incorporated into the ADA. See http://www.ada.gov/pubs/ada.htm for the
denition and specic changes to the text of the ADA. State laws and local ordinances may also
include individuals outside the Federal denition.
Durable Medical Equipment (DME)
Medical equipment (e.g., walkers, canes, wheelchairs, etc.) used by persons with a disability to
maintain their usual level of independence.
First Aid Station
Dedicated section in the shelter where residents receive rst aid and/or referrals for emergency
medical, mental, or dental health care.
Functional Needs Support Services (FNSS)
Services that enable children and adults to maintain their usual level of independence in a
general population shelter. FNSS includes reasonable modications to policies, practices, and
procedures, durable medical equipment (DME), consumable medical supplies (CMS), personal
assistance services (PAS), and other goods and services as needed. Children and adults requiring
FNSS may have physical, sensory, mental health, and cognitive and/or intellectual disabilities
affecting their ability to function independently without assistance. Others who may benet from
FNSS include women in late stages of pregnancy, elders, and those needing bariatric equipment.
Least restrictive environment
The opportunity for adults and children with disabilities and others with access or functional
needs to be with non-disabled peers to the greatest extent possible. These individuals should
have access to the general shelter activities or any other programs and services that non-disabled
persons can access. Generally, the less opportunity a person with a disability has to interact with
non-disabled persons (peers), the more the shelter (placement) is considered to be restricted.
Medical Staff
Licensed or certied physicians, registered nurses, licensed vocational nurses, emergency medical
technicians, and paramedics.
Mental Health Professional
A person who is licensed to provide counseling.
Personal Assistance Services
Services that assist children and adults with activities of daily living (e.g., bathing, toileting,
eating, etc.).
Service Animal
Any animal that is individually trained to provide assistance to a person with a disability.
43
Shelter
A temporary facility which provides housing and basic services until persons can return home or
obtain temporary or permanent house elsewhere.
Staff
People who are assigned a position in the shelter and who may or may not be paid for their
services.
Universal cot
A Universal/Accessible cot that meets the following recommended criteria:
• Height – 18”-19” without [below] the mattresses
• Width – minimum 27”
• Weight capacity – 350+ pounds
• Flexible head position
• Rails, if any, must be positioned or moveable in such a way as to allow for wheelchair
access (No IV pole)
Volunteers
Persons who are assigned staff positions in a shelter and meet the qualications of that position
but are not paid for their services.
44
7. Operational Tools *
Operational Tool #1 Planning Guidance
Operational Tool #2 Stakeholder Coordination
Operational Tool #3 Planning Shelter Capacity
Operational Tool #4 Locating the Shelter
Operational Tool #5 Evaluating the Shelter - Site Selection Tool
Operational Tool #6 Florida Shelter Selection Checklist
Operational Tool #7 San Jose California Shelter Assessment Checklist
Operational Tool #8 Durable Medical Equipment (DME) List
Operational Tool #9 Consumable Medical Supplies (CMS) List
Operational Tool #10 Communication Devices
Operational Tool #11 Resources for Assistive Technology
Operational Tool #12 Legal Authority - DME, CMS, Communication Devices
Operational Tool #13 Locating Services
Operational Tool #14 Documenting Service Providers
Operational Tool #15 Stafng the Shelter
Operational Tool #16 Assessment Teams
Operational Tool #17 Shelter Layout
Operational Tool #18 Dietary - Agreement
Operational Tool #19 Dietary - Menu
Operational Tool #20 Service Animals - Denition
Operational Tool #21 Communication - Strategies
Operational Tool #22 Communication - Devices
Operational Tool #23 Bathing and Toileting Ratios - Red Cross
Operational Tool #24 Mental Health Services
Operational Tool #25 Medical Station
Operational Tool #26 First Aid Station
Operational Tool #27 Medical Services - Form
Operational Tool #28 Medication
Operational Tool #29 Medication - Emergency Prescription Assistance Program (EPAP)
Operational Tool #30 Transportation Services
Operational Tool #31 Transportation Services - Form
Operational Tool #32 Transitioning Back to the Community
Operational Tool #33 Transitioning Back to the Community - Recovery
Operational Tool #34 Transitioning Back to the Community - Re-entry
Operational Tool #35 Closing the Shelter
Operational Tool #36 Closing the Shelter - Discharging Residents
Operational Tool #37 Closing the Shelter - Recovery
* Operational Tools – The operational tools in this document are excerpts and examples taken from
various agency and jurisdictional documents throughout the United States. While they are not meant
to dictate a State’s policies or procedures, they do present ideas and practices that can be adapted to t
each State’s specic needs.
45
8. Appendices
Page Appendix
47 Appendix 1 ADA Checklist for Emergency Shelters
115 Appendix 2 FORM: Contact Information for Shelter Services Providers
117 Appendix 3 Durable Medical Supply Sample List
118 Appendix 4 Consumable Medical Supply Sample List
125 Appendix 5 Guidance on Providing Personal Assistance Services
155 Appendix 6 One Day Menu for General Population Shelters Providing Functional
Needs Support Services
156 Appendix 7 FORM: Resident Health Care Information
158 Appendix 8 FORM: Medication Administration Record
160 Appendix 9 FORM: Transportation Request Information
162 Appendix 10 FORM: Resident Discharge Information
46
48
ADA Checklist for Emergency Shelters
$PHULFDQV ZLWK 'LVDELOLWLHV $FW
-XO\
86 'HSDUWPHQW RI -XVWLFH
&LYLO 5LJKWV 'LYLVLRQ
'LVDELOLW\ 5LJKWV 6HFWLR
Q

5HSURGXFWLRQ
5HSURGXFWLRQ RI WKLV GRFXPHQW LV HQFRXUDJHG
$GGLWLRQDO FRSLHV RI WKLV SXEOLFDWLRQ PD\ EH
REWDLQHG YLHZHG RU GRZQORDGHG IURP WKH
3XEOLFDWLRQV VHFWLRQ RI WKH $'$ :HEVLWH
ZZZDGDJRY RU E\ FDOOLQJ WKH $'$
,QIRUPDWLRQ /LQH DW YRLFH
77<
'LVFODLPHU
7KH $'$ DXWKRUL]HV WKH 'HSDUWPHQW RI -XVWLFH
WR SURYLGH WHFKQLFDO DVVLVWDQFH WR LQGLYLGXDOV
DQG HQWLWLHV WKDW KDYH ULJKWV RU UHVSRQVLELOLWLHV
XQGHU WKH $FW 7KLV GRFXPHQW SURYLGHV LQIRUPDO
JXLGDQFH WR DVVLVW \RX LQ XQGHUVWDQGLQJ WKH
$'$ DQG WKH 'HSDUWPHQW¶V UHJXODWLRQ
+RZHYHU WKLV WHFKQLFDO DVVLVWDQFH GRHV QRW
FRQVWLWXWH D OHJDO LQWHUSUHWDWLRQ RI WKH VWDWXWH
LL
7DEOH RI &RQWHQWV
LLL
ADA Checklist for Emergency Shelters ............................... 1
A. Evaluating the Physical
Accessibility of Emergency Shelters .................................... 1
B. Conducting Accessibility Surveys ........................................ 2
C. Getting Started ...................................................................... 2
D. Tools Needed .......................................................................... 3
E. Taking Measurements ........................................................... 3
1. Sloped Surfaces .............................................................. 3
2. Using the Tape Measure .................................................. 4
3. Measuring Door Openings .............................................. 5
F. Taking Photographs ................................................................ 5
G. Completing the Survey and Checklist .................................. 5
H. After Completing the Survey and Checklist ........................ 6
Step One: Accessible Shelter Quick-Check Survey ............ 7
Selecting Sites to Survey for Accessibility ..................................... 7
A. Accessible Entrance ............................................................. 7
B. Accessible Routes To All Service/Activity Areas ................. 8
C. Accessibility within Toilet Rooms ......................................... 10
Step Tw o
:
Ada Checklist For Emergency Shelters ............... 11
Getting to the Emergency Shelter .................................................. 11
A. Passenger Drop-Off Areas .................................................... 11
B. Parking ................................................................................... 14
1. Typical Issues .................................................................. 14
2. Parking Spaces Checklist ............................................... 15
3. Temporary Solutions for
Emergency Sheltering - Parking ................................... 18
C. Sidewalks and Walkways ...................................................... 19
1. Typical Issues for Individuals
Who Use Wheelchairs, Scooters,
or other Mobility Devices ............................................... 19
Accessible Ramp Features ......................................... 21
Temporary Solutions For Emergency
Sheltering - Ramps ..................................................... 22
2. Typical Issues for Individuals Who
Are Blind or Have Low Vision ........................................24
Temporary Solutions For Emergency
Sheltering - Protruding Object Hazards ................... 26
D. Entering the Emergency Shelter .......................................... 27
Building Entrance ............................................................... 27
E. Hallways and Corridors ........................................................ 30
1. Typical Issues for Individuals Who Use
Wheelchairs, Scooters, or Other Mobility Devices ....... 30
2. Typical Issues for People Who are Blind
or Have Low Vision ........................................................ 37
F. Check-In Areas ........................................................................ 39
Living at the Emergency Shelter ........................................... 40
G. Sleeping Areas ....................................................................... 40
H. Restrooms and Showers ....................................................... 42
Toilet Stalls ......................................................................... 46
I. Public Telephones ................................................................. 50
J. Drinking Fountains ............................................................... 52
K. Eating Areas .......................................................................... 54
Other Issues ............................................................................ 56
L. Availability of Electrical Power ............................................ 56
M. Single-User or “Family” Toilet Room ................................. 57
N. Health Units/Medical Care Areas ........................................ 62
O. Accessible Portable Toilets ................................................... 63
ACCESSIBLE EMERGENCY SHELTERS
2QH RI WKH PRVW LPSRUWDQW UROHV RI 6WDWH DQG ORFDO JRYHUQPHQW
LV WR SURWHFW SHRSOH IURP KDUP LQFOXGLQJ KHOSLQJ SHRSOH REWDLQ
IRRG DQG VKHOWHU LQ PDMRU HPHUJHQFLHV :KHQ GLVDVWHUV RFFXU
SHRSOH DUH RIWHQ SURYLGHG VDIH UHIXJH LQ WHPSRUDU\ VKHOWHUV ORFDWHG
LQ VFKRROV RIÀFH EXLOGLQJV WHQWV RU RWKHU IDFLOLWLHV $GYDQFH
SODQQLQJ IRU DQ HPHUJHQF\ VKHOWHU W\SLFDOO\ LQYROYHV HQVXULQJ WKDW
WKH VKHOWHU ZLOO EH ZHOO VWRFNHG ZLWK EDVLF QHFHVVLWLHV VXFK DV IRRG
ZDWHU DQG EODQNHWV 3ODQQLQJ VKRXOG DOVR LQYROYH HQVXULQJ WKDW
WKHVH VKHOWHUV DUH DFFHVVLEOH WR SHRSOH ZLWK GLVDELOLWLHV 0DNLQJ
HPHUJHQF\ VKHOWHULQJ SURJUDPV DFFHVVLEOH LV JHQHUDOO\ UHTXLUHG E\
WKH $PHULFDQV ZLWK 'LVDELOLWLHV $FW RI $'$
A. Evaluating the Physical Accessibility of Emergency Shelters
,Q RUGHU WR EH SUHSDUHG IRU DQ HPHUJHQF\ WKDW UHTXLUHV VKHOWHULQJ
DFFHVVLEOH IHDWXUHV VKRXOG EH SDUW RI DQ HPHUJHQF\ VKHOWHU $ ÀUVW
VWHS WR SURYLGLQJ DQ DFFHVVLEOH VKHOWHU LV WR LGHQWLI\ DQ\ SK\VLFDO
EDUULHUV WKDW H[LVW WKDW ZLOO SUHYHQW DFFHVV WR SHRSOH ZLWK GLVDELOLWLHV
2QH JRRG ZD\ WR GR WKLV LV WR LQVSHFW HDFK VKHOWHU IDFLOLW\ WKDW \RXU
FRPPXQLW\ SODQV WR XVH LQ DQ HPHUJHQF\ DQG LGHQWLI\ EDUULHUV WR
SHRSOH ZLWK GLVDELOLWLHV LQFOXGLQJ SHRSOH ZKR XVH ZKHHOFKDLUV RU
VFRRWHUV RU ZKR KDYH GLIÀFXOW\ ZDONLQJ SHRSOH ZKR DUH GHDI RU
KDUGRIKHDULQJ DQG SHRSOH ZKR DUH EOLQG RU ZKR KDYH ORZ YLVLRQ
)DFLOLWLHV EXLOW RU H[WHQVLYHO\ DOWHUHG VLQFH WKH $'$ ZHQW LQWR HIIHFW
LQ PD\ KDYH IHZ EDUULHUV WR DFFHVVLELOLW\ DQG FRXOG EH JRRG
FKRLFHV IRU HPHUJHQF\ VKHOWHUV )DFLOLWLHV EXLOW EHIRUH DQG QRW
DOWHUHG WR SURYLGH DFFHVVLELOLW\ PD\ KDYH EDUULHUV WKDW SUHYHQW DFFHVV
WR SHRSOH ZLWK GLVDELOLWLHV
:KHQ HYDOXDWLQJ SK\VLFDO DFFHVVLELOLW\ LQ ROGHU IDFLOLWLHV LW PD\ EH
D JRRG LGHD WR GR WKH DQDO\VLV LQ WZR SDUWV ,I \RX VXVSHFW WKDW DQ
ROGHU IDFLOLW\ LV QRW DFFHVVLEOH \RX FDQ GR D SUHOLPLQDU\ DQDO\VLV
EHIRUH FRPSOHWLQJ D GHWDLOHG DFFHVVLELOLW\ VXUYH\ 7KLV SUHOLPLQDU\
DQDO\VLV RU TXLFNFKHFN FDQ HOLPLQDWH IDFLOLWLHV ZLWK H[WHQVLYH
EDUULHUV VR WKDW WKH IRFXV FDQ EH RQ WKRVH IDFLOLWLHV WKDW DUH PRVW
DSSURSULDWH WR EHFRPH DFFHVVLEOH VKHOWHUV 7R KHOS LGHQWLI\ ROGHU
1
ADA Emergency Shelter Checklist

EXLOGLQJV WKDW PD\ EH JRRG FDQGLGDWHV WR EHFRPH DFFHVVLEOH
VKHOWHUV D FRS\ RI WKH $FFHVVLEOH 6KHOWHU 4XLFN&KHFN 6XUYH\ LV
SURYLGHG RQ SDJH $IWHU FRPSOHWLQJ WKH 4XLFN&KHFN 6XUYH\
LI \RX KDYH FKHFNHG ´<H Vµ IRU PRVW RI WKH TXHVWLRQV RQ WKH IRUPV
\RX VKRXOG FRQGXFW D IXOO DFFHVVLELOLW\ VXUYH\ XVLQJ WKH $'$
&KHFNOLVW IRU (PHUJHQF\ 6KHOWHUV
,I \RX ÀQG EDUULHUV WR DFFHVVLELOLW\ DIWHU FRPSOHWLQJ WKH FKHFNOLVW
WKH QH[W VWHS LV WR HLWKHU UHPRYH WKH EDUULHUV RU LGHQWLI\ RWKHU
QHDUE\ DFFHVVLEOH IDFLOLWLHV WKDW FDQ VHUYH DV D VKHOWHU ,Q
FRPPXQLWLHV ZLWK PRUH WKDQ RQH HPHUJHQF\ VKHOWHU XQWLO DOO
VKHOWHUV DUH DFFHVVLEOH WKH ORFDWLRQV RI DFFHVVLEOH VKHOWHUV VKRXOG
EH ZLGHO\ SXEOLFL]HG SDUWLFXODUO\ WR SHRSOH ZLWK GLVDELOLWLHV DQG
RUJDQL]DWLRQV WKDW VHUYH WKH GLVDELOLW\ FRPPXQLW\
B. Conducting Accessibility Surveys
7KH IROORZLQJ 4XLFN&KHFN 6XUYH\ EHJLQQLQJ RQ SDJH DQG
WKH $'$ &KHFNOLVW IRU (PHUJHQF\ 6KHOWHUV EHJLQQLQJ RQ SDJH
DUH GHVLJQHG WR DVVLVW 6WDWH DQG ORFDO RIÀFLDOV DQG RSHUDWRUV RI
HPHUJHQF\ VKHOWHUV WR GHWHUPLQH ZKHWKHU D IDFLOLW\ EHLQJ FRQVLGHUHG
IRU XVH DV DQ HPHUJHQF\ VKHOWHU LV DFFHVVLEOH DQG LI QRW ZKHWKHU
PRGLÀFDWLRQV DUH QHHGHG WR UHPRYH EDUULHUV RU ZKHWKHU UHORFDWLRQ WR
DQRWKHU DFFHVVLEOH IDFLOLW\ LV QHFHVVDU\ )LOOLQJ RXW WKH 4XLFN&KHFN
6XUYH\ ZLOO SURYLGH JXLGDQFH RQ ZKHWKHU D IDFLOLW\ KDV FHUWDLQ EDVLF
DFFHVVLEOH IHDWXUHV DQG ÀOOLQJ RXW WKH GHWDLOHG $'$ &KHFNOLVW IRU
(PHUJHQF\ 6KHOWHUV ZLOO SURYLGH VSHFLÀF LQIRUPDWLRQ RQ DQ\ EDUULHUV
WR DFFHVVLELOLW\
C. Getting Started
,QGLYLGXDOV FRQGXFWLQJ WKH VXUYH\V QHHG QRW EH H[SHULHQFHG LQ
HYDOXDWLQJ IDFLOLWLHV IRU DFFHVVLELOLW\ 7KH FKHFNOLVW SURYLGHV
JXLGDQFH RQ KRZ WR FRPSOHWH WKH VXUYH\ DQG ZLOO SURPSW WKH XVHU
WR FKHFN NH\ HOHPHQWV 7KH FKHFNOLVW SDJHV DOVR SURYLGH VSDFH IRU
QRWHV DQG RWKHU NH\ LQIRUPDWLRQ 7KH FKHFNOLVW LV GHVLJQHG WR SURPSW
WKH XVHU WR FKHFN NH\ IHDWXUHV E\ DVNLQJ TXHVWLRQV DERXW VL]HV VORSHG
VXUIDFHV DQG DYDLODELOLW\ RI DFFHVVLEOH IHDWXUHV DQG LQ VRPH DUHDV LW
VXJJHVWV DOWHUQDWLYHV LI D SK\VLFDO EDUULHU LV LGHQWLÀHG %\ IROORZLQJ
WKH GLUHFWLRQV SURYLGHG IRU ÀOOLQJ RXW WKH FKHFNOLVW VWDII FDQ LGHQWLI\
DFFHVVLEOH VKHOWHUV DQG GHYHORS LQIRUPDWLRQ QHHGHG WR LPSOHPHQW
WHPSRUDU\ DQG SHUPDQHQW DFFHVVLELOLW\ PRGLÀFDWLRQV
$Q HYDOXDWLRQ RI VKHOWHU DFFHVVLELOLW\ VKRXOG IRFXV RQ WKRVH DUHDV RI
WKH IDFLOLW\ WKDW PD\ EH XVHG IRU SURYLGLQJ VKHOWHU LQ DQ HPHUJHQF\
7KHVH LQFOXGH DUHDV ZKHUH SHRSOH DUH GURSSHG RII E\ D EXV YDQ RU
FDU WKH SDUNLQJ DUHD WKH HQWUDQFH WR WKH VKHOWHU SHGHVWULDQ URXWHV
ERWK H[WHULRU DQG LQWHULRU VOHHSLQJ HDWLQJ LQIRUPDWLRQ DQG
UHFUHDWLRQDO DUHDV DQG WRLOHW URRPV
%HIRUH VKHOWHU DFFHVVLELOLW\ LV HYDOXDWHG LW LV XVHIXO IRU VWDII WR
UHYLHZ WKH LQVWUXFWLRQV IRU ÀOOLQJ RXW WKH FKHFNOLVW DQG EHFRPH
IDPLOLDU ZLWK WKH TXHVWLRQV ,W LV DOVR KHOSIXO WR SUDFWLFH WDNLQJ
PHDVXUHPHQWV SKRWRJUDSKV DQG UHFRUGLQJ LQIRUPDWLRQ
2Q WKH GD\ RI WKH VXUYH\ LW LV KHOSIXO WR ÀUVW EHFRPH IDPLOLDU ZLWK
FHUWDLQ DUHDV EHIRUH VWDUWLQJ WR UHFRUG LQIRUPDWLRQ 8SRQ DUULYDO DW
WKH SURSRVHG VKHOWHU ÀUVW ÀQG WKH DUHDV ZKHUH SHRSOH ZLOO GLVHPEDUN
IURP YHKLFOHV ERWK SDVVHQJHU GURSRII DQG ORDGLQJ ]RQHV DV ZHOO
2
ADA Emergency Shelter Checklist
DV SDUNLQJ DUHDV 1H[W ÀQG WKH HQWUDQFHV WR WKH VKHOWHU DUHDV WKDW
ZLOO EH XVHG GXULQJ DQ HYDFXDWLRQ ,I SRVVLEOH WDNH DQ LGHQWLI\LQJ
´ORFDWLRQµ SKRWRJUDSK WKDW VKRZV WKH QDPH RI WKH IDFLOLW\ DQG WKH
DGGUHVV VR WKDW RWKHU SKRWRJUDSKV FDQ EH LGHQWLÀHG FRUUHFWO\ :KHQ
LQVLGH WKH EXLOGLQJ ORFDWH WKH DUHDV ZKHUH SHRSOH DUH OLNHO\ WR
UHJLVWHU VOHHS DQG HDW /RFDWH WKH WRLOHW URRPV WKDW VHUYH WKH VKHOWHU
DUHD ,W LV DOVR D JRRG LGHD WR ORFDWH DQ\ DUHDV XVHG IRU WHOHSKRQHV
IRRG GLVWULEXWLRQ DQG PHGLFDO VHUYLFHV
D. Tools Needed
7KH IROORZLQJ LWHPV DUH QHHGHG IRU WKH VXUYH\
$ PHWDO WDSH PHDVXUH WKDW LV DW OHDVW IHHW ORQJ
$ GLJLWDO OHYHO RU EXEEOH OHYHO WKDW LV LQFKHV ORQJ
$ GRRU SUHVVXUH JDXJH
$ GLJLWDO SUHIHUUHG RU ¿OP FDPHUD ZLWK D ÀDVK
2QH FRS\ RI WKH FKHFNOLVW IRU HDFK VKHOWHU
DQG 4XLFN&KHFN 6XUYH\ LI XVHG DQG
$ FOLSERDUG DQG SHQV
,I \RX DUH QRW IDPLOLDU ZLWK WDNLQJ WKH W\SHV RI PHDVXUHPHQWV QHHGHG
WR FRPSOHWH WKH FKHFNOLVW UHYLHZ WKH IROORZLQJ VHFWLRQ DQG SUDFWLFH
XVLQJ WKH WRROV EHIRUH JRLQJ WR FRQGXFW D VXUYH\
E. Taking Measurements
1. Sloped Surfaces
0HDVXULQJ WKH VORSH RI D UDPS SDUNLQJ VSDFH ZDONZD\ RU RWKHU
JURXQG RU ÁRRU VXUIDFH LV LPSRUWDQW WR LGHQWLI\ ZKHWKHU WKH VXUIDFH LV
DFFHVVLEOH 7KH DPRXQW RI VORSH RU JUDGH LV GHVFULEHG DV WKH SURSRU
WLRQ RI D YHUWLFDO ULVH WR D KRUL]RQWDO OHQJWK ,W LV XVXDOO\ GHVFULEHG
DV
D UDWLR HJ ZKLFK PHDQV RQH XQLW RI YHUWLFDO ULVH IRU
HDFK XQLWV RI KRUL]RQWDO OHQJWK RU
D SHUFHQWDJH HJ ZKLFK HTXDWHV WR D UDWLR RI RU
GHJUHHV
7KH HDVLHVW ZD\ WR PHDVXUH VORSH LV WR XVH D GLJLWDO OHYHO 7KH GLJLWDO
GLVSOD\ JLYHV D UHDGLQJ WKDW PD\ EH VKRZQ DV D SHUFHQW GHJUHHV
RU DV D GLJLWDO EXEEOH %HIRUH XVLQJ D GLJLWDO OHYHO PDNH VXUH WR
XQGHUVWDQG WKH GLUHFWLRQV IRU LWV XVH ,W ZLOO QHHG WR EH FDOLEUDWHG
EHIRUH HDFK XVH 7KH PD[LPXP UXQQLQJ VORSH JHQHUDOO\ DOORZHG
IRU UDPSV LV RU GHJUHHV &URVV VORSH LV WKH VORSH
RU JUDGH RI D VXUIDFH SHUSHQGLFXODU WR WKH UXQQLQJ VORSH 7KH PRVW
FURVV VORSH DOORZHG RQ DQ DFFHVVLEOH URXWH LV RU
GHJUHHV
3
ADA Emergency Shelter Checklist
2. Using the Tape Measure
$ PHWDO WDSH PHDVXUH LV QHHGHG WR PHDVXUH WKH OHQJWK ZLGWK KHLJKW DQG GHSWK
RI YDULRXV HOHPHQWV :KHQ PHDVXULQJ ORQJ GLVWDQFHV SXOO WKH WDSH WLJKW WR JHW
DQ DFFXUDWH PHDVXUHPHQW 7KH FKHFNOLVW ZLOO RIIHU JXLGDQFH IRU WKH VSHFL¿F
PHDVXUHPHQW WKDW LV UHTXLUHG
Using a tape measure to measure the width of a
parking space
$QRWKHU ZD\ WR PHDVXUH VORSH WKDW UHTXLUHV PRUH HIIRUW LV WR XVH D LQFK OHYHO
ZLWK OHYHOLQJ EXEEOH DQG D PHWDO WDSH PHDVXUH 3ODFH WKH OHYHO RQ WKH VORSHG
VXUIDFH LQ WKH GLUHFWLRQ \RX ZLVK WR PHDVXUH 5HVW RQH HQG RI WKH OHYHO DW WKH
KLJKHVW SRLQW RI WKH VORSHG VXUIDFH DQG OLIW WKH RWKHU HQG VHH EHORZ XQWLO WKH
EXEEOH LV LQ WKH PLGGOH RI WKH WXEH 7KLV LV WKH ´OHYHOµ SRVLWLRQ :KLOH WKH OHYHO LV
LQ WKLV SRVLWLRQ PHDVXUH WKH GLVWDQFH EHWZHHQ WKH HQG RI WKH OHYHO DQG WKH VORSHG
VXUIDFH EHORZ ,I WKH GLVWDQFH LV WZR LQFKHV RU OHVV WKHQ WKH VORSH LV RU OHVV
:KHQ WKH GLVWDQFH LV PRUH WKDQ WZR LQFKHV UHFRUG WKH GLVWDQFH RQ WKH FKHFNOLVW VR
WKH H[DFW VORSH FDQ EH FDOFXODWHG ODWHU )RU PHDVXULQJ FURVV VORSH LI WKH GLVWDQFH
PHDVXUHG IURP WKH OHYHO SRVLWLRQ LV ô LQFK RU OHVV WKHQ WKH VORSH LV RU OHVV
Measuring slope using a 24-inch bubble level
and tape measure
4
ADA Emergency Shelter Checklist
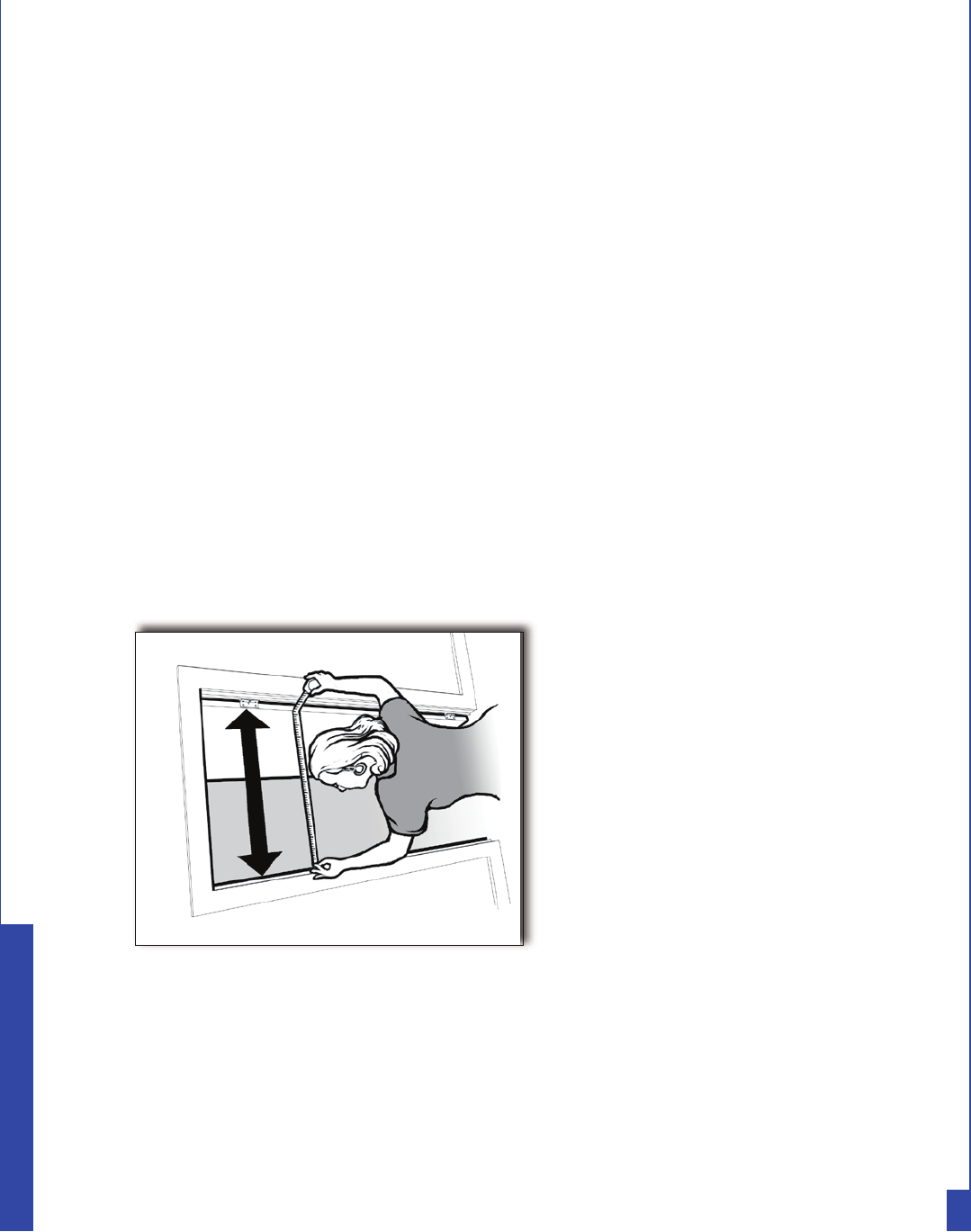
3. Measuring Door Openings
6SHFLDO FDUH LV QHHGHG ZKHQ
PHDVXULQJ WKH FOHDU RSHQLQJ
RI D GRRUZD\ 7R PHDVXUH
WKH FOHDU RSHQLQJ RI D
VWDQGDUG KLQJHG GRRU RSHQ
WKH GRRU WR GHJUHHV 3ODFH
WKH HQG RI WKH WDSH PHDVXUH
RQ WKH VLGH RI WKH GRRU IUDPH
QH[W WR WKH FOHDU RSHQLQJ
VHH EHORZ 6WUHWFK WKH WDSH
DFURVV WKH GRRU RSHQLQJ WR
WKH IDFH RI WKH GRRU 7KLV
PHDVXUHV WKH FOHDU ZLGWK RI
WKH GRRU RSHQLQJ WKURXJK
ZKLFK SHRSOH SDVV ZKLFK
LV OHVV WKDQ WKH ZLGWK RI WKH
GRRU LWVHOI
F. Taking Photographs
$ FRPSUHKHQVLYH VHW RI SKRWRJUDSKV PDNHV LW HDVLHU WR XQGHUVWDQG
H[LVWLQJ FRQGLWLRQV DIWHU WKH VXUYH\ LV FRPSOHWHG ,W LV D JRRG LGHD
WR WDNH PDQ\ SKRWRV RI WKH H[WHULRU DQG LQWHULRU RI WKH SRWHQWLDO
VKHOWHU ,W LV OLNHO\ WKDW PDQ\ RWKHU SHRSOH LQ \RXU GHFLVLRQPDNLQJ
SURFHVV ZLOO QHHG WR UHYLHZ LQIRUPDWLRQ DERXW WKH IDFLOLW\ \RX DUH
VXUYH\LQJ VR WU\ WR UHFRUG HDFK HOHPHQW WKDW \RX VXUYH\ ZLWK VHYHUDO
SKRWRV ,W LV DOZD\V XVHIXO WR ÀUVW WDNH D SKRWR WKDW ZLOO FOHDUO\
Measuring the clear opening from
the face of the doorstop on the
frame to the face of the open door
LGHQWLI\ WKH ORFDWLRQ RI WKH HOHPHQW VR WKDW RWKHUV ZLOO HDVLO\ EH DEOH
WR ÀQG WKH HOHPHQW 7KHQ WDNH VHYHUDO FORVHXS VKRWV RI WKDW HOHPHQW
WR GRFXPHQW WKH FRQGLWLRQV \RX IRXQG GXULQJ \RXU VXUYH\ ,I \RX
DUH QRW IDPLOLDU ZLWK WKH FDPHUD WKDW \RX SODQ WR XVH SUDFWLFH XVLQJ
LW ERWK LQGRRUV DQG RXWGRRUV EHIRUH VWDUWLQJ WR VXUYH\ WKH YDULRXV
IDFLOLWLHV EHLQJ FRQVLGHUHG IRU XVH DV VKHOWHUV ,I \RX DUH XVLQJ D
GLJLWDO FDPHUD LW LV D JRRG LGHD WR UHYLHZ WKH LPDJHV DV \RX WDNH
WKHP WR HQVXUH WKDW \RX KDYH JRRG TXDOLW\ SKRWRJUDSKV
G. Completing the Survey and Checklist
7KH VXUYH\ DQG FKHFNOLVW IRUPV ZLOO SURPSW \RX IRU ZKDW WR ORRN
DW DQG ZKHUH WR PHDVXUH <RX VKRXOG ZULWH GRZQ DOO DQVZHUV DQG
QRWHV IRU XVH ODWHU LQ WKH SODQQLQJ SURFHVV ,I D SKRWR LV WDNHQ RI
D SDUWLFXODU HOHPHQW RU FRQGLWLRQ WKHQ \RX VKRXOG QRWH WKLV RQ WKH
FKHFNOLVW ,W LV XVXDOO\ PRUH HIÀFLHQW IRU WZR RU WKUHH SHRSOH WR ZRUN
WRJHWKHU GRLQJ WKHVH VXUYH\V 2QH SHUVRQ FDQ PHDVXUH ZKLOH WKH
RWKHU UHFRUGV WKH LQIRUPDWLRQ DQG WDNHV SKRWRV
)RU HDFK LWHP FKHFN HLWKHU ´<HVµ RU ´1Rµ ,I WKH PHDVXUHPHQW
RU QXPEHU IDOOV VKRUW RI WKDW UHTXLUHG IRU DFFHVVLELOLW\ ZULWH WKH
PHDVXUHPHQW RU QXPEHU WR WKH ULJKW RI WKH TXHVWLRQ $GG QRWHV RU
FRPPHQWV DV QHHGHG )RU VRPH TXHVWLRQV ZKHQ ´1Rµ LV WKH DQVZHU
WKH FKHFNOLVW ZLOO LQFOXGH D SURPSW WR FKHFN IRU DQ DOWHUQDWH VROXWLRQ
,QIRUPDWLRQ RQ SRVVLEOH DOWHUQDWLYH VROXWLRQV FDQ EH XVHG ODWHU WR
GHFLGH KRZ WR EHWWHU SURYLGH DFFHVVLELOLW\ 7DNLQJ VHYHUDO SKRWRV
LV DOVR KHOSIXO ZKHQ WKH DQVZHU LV ´1Rµ DQG DQ DOWHUQDWLYH ZD\ WR
SURYLGH DFFHVVLELOLW\ LV QRW UHDGLO\ DSSDUHQW
5
ADA Emergency Shelter Checklist
:KHQ FRPSOHWLQJ WKH VXUYH\ RU FKHFNOLVW WU\ WR DQVZHU HYHU\
TXHVWLRQ LQ HDFK VHFWLRQ XQOHVV WKH HOHPHQW LV QRW SUHVHQW DW WKDW
IDFLOLW\ )RU H[DPSOH LI QR SDUNLQJ ORW LV SURYLGHG DW WKH IDFLOLW\
VXFK DV ZKHUH RQO\ RQVWUHHW SDUNLQJ LV SURYLGHG GR QRW PHDVXUH
WKH VL]H RI WKH RQVWUHHW SDUNLQJ VSDFHV
6RPH VHFWLRQV RI WKH FKHFNOLVW DUH GLYLGHG LQWR WZR SDUWV RQH IRU
LQGLYLGXDOV ZLWK D PRELOLW\ GLVDELOLW\ DQG WKH RWKHU IRU LQGLYLGXDOV
ZKR DUH EOLQG RU ZKR KDYH ORZ YLVLRQ :KLOH HYDOXDWLQJ D IDFLOLW\
\RX ZLOO EH FKHFNLQJ WR HQVXUH WKDW DQ DFFHVVLEOH URXWH LV SURYLGHG
7KH DFFHVVLEOH URXWH LV D FRQWLQXRXV XQREVWUXFWHG SHGHVWULDQ SDWK
ZLWKRXW VWHSV RU VWHHS VORSHV WKDW FRQQHFWV DOO DFFHVVLEOH VLWH DQG
EXLOGLQJ IHDWXUHV DQG VSDFHV WRJHWKHU $ FRQWLQXRXV DFFHVVLEOH URXWH
PXVW EH DYDLODEOH DW WKH VKHOWHU IRU SHRSOH ZKR XVH D ZKHHOFKDLU
VFRRWHU RU RWKHU PRELOLW\ GHYLFH 2WKHU VHFWLRQV RI WKH FKHFNOLVW DVN
TXHVWLRQV UHODWHG WR LQGLYLGXDOV ZKR DUH EOLQG RU KDYH ORZ YLVLRQ
7KHVH TXHVWLRQV FRYHU DOO FLUFXODWLRQ SDWKV QRW MXVW SHGHVWULDQ SDWKV
WKDW DUH DOVR DQ DFFHVVLEOH URXWH
7KH VXUYH\ DQG WKH FKHFNOLVW DUH EDVHG RQ VRPH RI WKH UHTXLUHPHQWV
IURP WKH $'$ 6WDQGDUGV IRU $FFHVVLEOH 'HVLJQ WKH 6WDQGDUGV
4XHVWLRQV KDYH EHHQ VHOHFWHG WR UHÁHFW IHDWXUHV WKDW PD\ EH PRVW
LPSRUWDQW IRU WKH VKRUWWHUP VWD\V FRPPRQ IRU HPHUJHQF\ VKHOWHUV
7R OHDUQ PRUH DERXW WKH 6WDQGDUGV VHH WKH 'HSDUWPHQW RI -XVWLFH
UHJXODWLRQV &)5 3DUW $SSHQGL[ $ 7KH UHJXODWLRQV DQG WKH
6WDQGDUGV DUH DYDLODEOH DW ZZZDGDJRY &RSLHV DUH DOVR DYDLODEOH
E\ FDOOLQJ WKH $'$ ,QIRUPDWLRQ /LQH DW YRLFH RU
77<
H. After Completing the Survey and Checklist
2QFH \RX KDYH FRPSOHWHG WKH VXUYH\ DQG ¿OOHG RXW WKH FKHFNOLVW
\RX FDQ GHWHUPLQH ZKLFK HOHPHQWV RU VSDFHV LQ D SRWHQWLDO VKHOWHU
IDFLOLW\ DUH DFFHVVLEOH DQG ZKLFK PD\ QHHG PRGL¿FDWLRQV ,I PRVW
DQVZHUV DUH ³\HV´ WKH IDFLOLW\ PD\ QHHG OLWWOH RU QR PRGL¿FDWLRQ
,I VRPH DQVZHUV DUH ³QR´ PRGL¿FDWLRQV PD\ EH QHHGHG WR UHPRYH
EDUULHUV IRXQG LQ WKDW VSDFH RU HOHPHQW (PHUJHQF\ VKHOWHUV LQ ROGHU
EXLOGLQJV ZLWK LQDFFHVVLEOH IHDWXUHV PLJKW EH PDGH DFFHVVLEOH ZLWK
WHPSRUDU\ PRGL¿FDWLRQV VXFK DV SRUWDEOH UDPSV DW WKH HQWUDQFH
DQG DFFHVVLEOH SDUNLQJ VSDFHV PDUNHG RII E\ WUDI¿F FRQHV XQWLO
SHUPDQHQW PRGL¿FDWLRQV FDQ EH PDGH +RZHYHU ZKHUH IDFLOLWLHV DUH
QRW FDSDEOH RI EHLQJ PDGH DFFHVVLEOH DQRWKHU IDFLOLW\ ZLOO QHHG WR EH
VHOHFWHG IRU XVH DV D VKHOWHU
6
ADA Emergency Shelter Checklist
Step One: Accessible Shelter Quick-Check Survey
Yes _____ No _____
Yes _____ No _____
A. Accessible Entrance
+DYLQJ D ZD\ WR JHW LQWR WKH HPHUJHQF\ VKHOWHU RQ D VXUIDFH WKDW LV ÀUP VWDEOH VOLS
UHVLVWDQW ZLWKRXW VWHSV RU VWHHS VORSHV DQG ZLGH HQRXJK IRU D SHUVRQ XVLQJ D ZKHHOFKDLU
RU RWKHU PRELOLW\ DLG LV HVVHQWLDO
A1. Is there a sidewalk connecting the parking area and any drop off area to
the walkway leading to the building? [ADA Standards § 4.1.3(1)]
A2. Is there a route without steps from this sidewalk to the main entrance?
If No, are there two or fewer steps? Yes _____ No ____ Number of Steps: _____
If No, is there another entrance without steps that is connected by a sidewalk to the
parking or drop off area? Yes _____ No _____Location: ______________________________
_________________________________________________________
Selecting Sites to Survey for Accessibility
3URYLGLQJ DQ HPHUJHQF\ VKHOWHU WKDW LV DFFHVVLEOH WR SHRSOH ZLWK GLVDELOLWLHV LQYROYHV PDNLQJ VXUH WKDW D QXPEHU
RI DFFHVVLEOH IHDWXUHV DQG VSDFHV DUH DYDLODEOH 7R YHULI\ DFFHVVLELOLW\ EHIRUH GHFLGLQJ RQ D VLWH IRU DQ HPHUJHQF\
VKHOWHU FDQ LQYROYH DVNLQJ PDQ\ TXHVWLRQV VXFK DV WKRVH LQ WKH $'$ &KHFNOLVW IRU (PHUJHQF\ 6KHOWHUV )RU VRPH
ROGHU EXLOGLQJV HVSHFLDOO\ WKRVH RQ KLOO\ VLWHV DQG WKRVH WKDW KDYH QRW EHHQ UHQRYDWHG UHPRGHOHG RU DOWHUHG VLQFH
EHIRUH FRPSOHWLQJ WKH GHWDLOHG FKHFNOLVW LW PD\ EH EHWWHU WR GR D SUHWHVW WKDW FDQ UXOH RXW D IDFLOLW\ ZLWK
PDMRU DFFHVVLELOLW\ SUREOHPV VR DYDLODEOH UHVRXUFHV FDQ EH IRFXVHG RQ RWKHU ORFDWLRQV 7KH IROORZLQJ TXHVWLRQV
ZLOO KHOS HYDOXDWH ZKHWKHU D IDFLOLW\ KDV VXFK PDMRU DFFHVVLELOLW\ EDUULHUV $IWHU WKLV ÀUVW VWHS EXLOGLQJV WKDW
GR QRW KDYH PDMRU DFFHVVLELOLW\ SUREOHPV VKRXOG EH VXUYH\HG PRUH WKRURXJKO\ XVLQJ WKH $'$ &KHFNOLVW IRU
(PHUJHQF\ 6KHOWHUV WR ÀQG RXW ZKLFK LI DQ\ EDUULHUV QHHG WR EH UHPRYHG WR SURYLGH DQ DFFHVVLEOH VKHOWHU
7
Accessible Quick-Check Survey
Notes/Comments
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
B. Accessible Routes To All Service/Activity Areas
(YHU\RQH PXVW EH DEOH WR JHW WR HDFK RI WKH YDULRXV DUHDV ZKHUH DFWLYLWLHV DQG VHUYLFHV
WDNH SODFH 7KLV LQFOXGHV SHRSOH ZKR XVH PRELOLW\ GHYLFHV VXFK DV ZKHHOFKDLUV DQG
VFRRWHUV EHLQJ DEOH WR JHW WR ORFDWLRQV ZKHUH VXSSOLHV DUH GLVWULEXWHG WR HDWLQJ DUHDV WR
VOHHSLQJ DUHDV WR WRLOHW URRPV DQG WR RWKHU DFWLYLW\ DUHDV ZLWKRXW HQFRXQWHULQJ VWDLUV RU
VWHHS VORSHV
&KHFN DOO RI WKH YDULRXV ZD\V WR JHW WR HDFK RI WKH DUHDV ZKHUH VKHOWHULQJ DFWLYLWLHV DUH
OLNHO\ WR WDNH SODFH VOHHSLQJ HDWLQJ VXSSO\ GLVWULEXWLRQ EDWKURRPV HWF
B1. Sleeping Area (Location: ______________________________________)
B1-a. Is there a route without steps from the accessible entrance to this
location?
If No, are there two or fewer steps? Yes ___ No ___Number of Steps: _______
If No, is there a ramp, lift, or elevator? Yes ___ No ___Type of device: _______
B1-b. If an elevator or lift provides the only accessible route, is there
a source of backup power to operate the device for an extended
period?
B2. Eating Area (Location: ______________________________________)
B2-a. Is there a route without steps from the accessible entrance to this
location?
If No, are there two or less steps? Yes ___ No ____ Number of Steps: _____
If No, is there a ramp, lift, or elevator? Yes ___ No ____ Type of device: _______
8
Accessible Quick-Check Survey
B2-b. If an elevator or lift provides the only accessible route, is there a
source of back up power to operate the device for an extended
period?
B3. Supply Distribution Area (Location: _____________________________)
B3-a. Is there a route without steps from the accessible entrance to this
location?
If No, are there two or fewer steps? Yes ___ No ___ Number of Steps: ______
If No, is there a ramp, lift, or elevator? Yes ___ No ___ Type of device: ______
B3-b. If an elevator or lift provides the only accessible route, is there
a source of backup power to operate the device for an extended
period?
B4. Toilet Rooms (Location: ________________________________________)
B4-a. Is there a route without steps from the accessible entrance to this
location?
If No, are there two or fewer steps? Yes ___ No ____ Number of Steps: ______
If No, is there a ramp, lift, or elevator? Yes ____ No ____ Type of device: ______
B4-b. If an elevator or lift provides the only accessible route, is there
a source of backup power to operate the device for an extended
period?
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
9
Accessible Quick-Check Survey
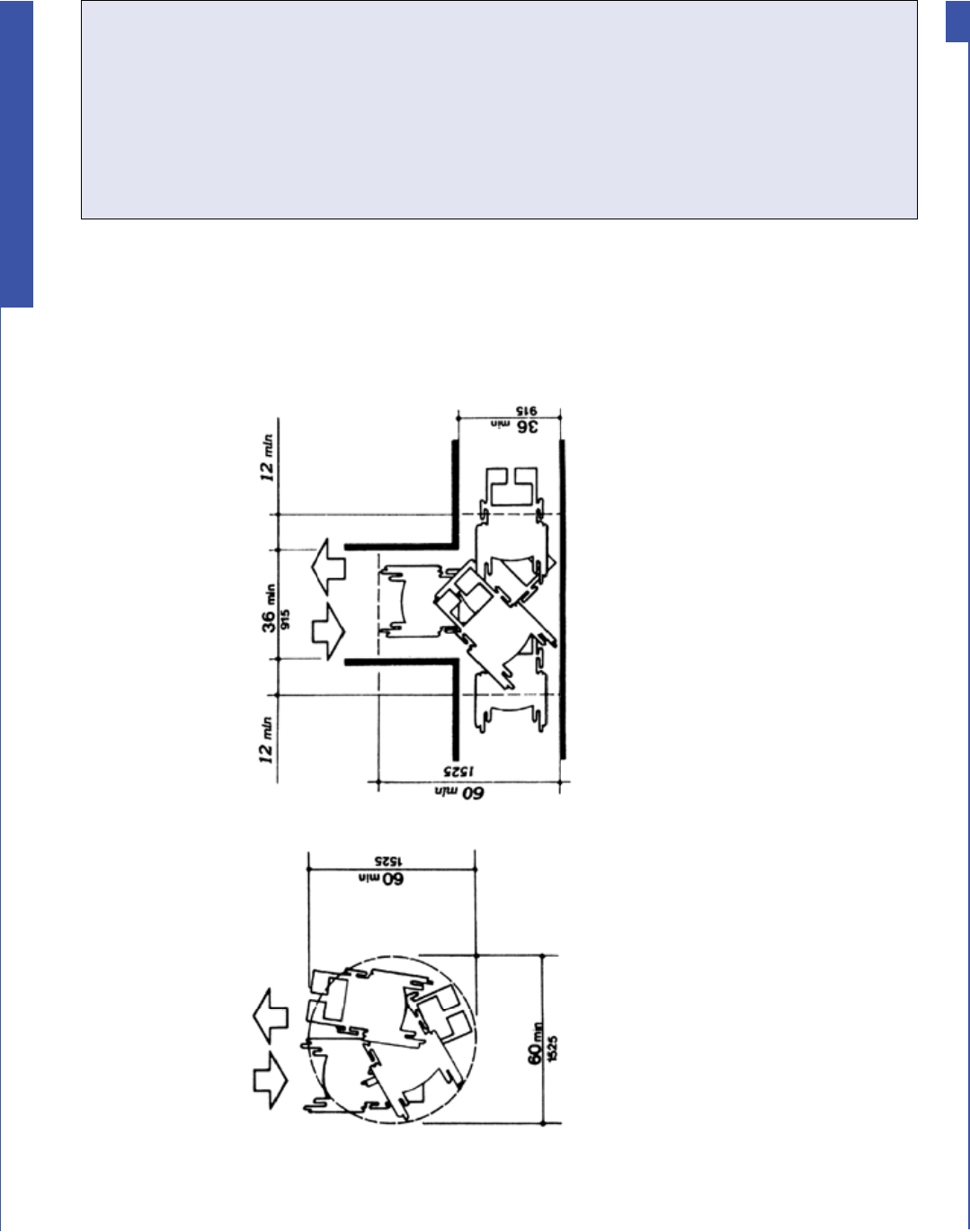
C. Accessibility Within Toilet Rooms
C1-a. Is there an area within the toilet room where a person who
uses a wheelchair or mobility device can turn around - either
a minimum 60-inch diameter circle or a “T”-shaped turn area?
[ADA Standards §§ 4.22.3; 4.2.3, Fig. 3]
C1-b. Is at least one stall at least 60 inches wide and 56 inches deep
(wall mounted toilet) or 59 inches deep (floor mounted toilet)?
[ADA Standards § 4.17.3]
Fig 3
Minimum spaces for turning
8VLQJ 7KH ,QIRUPDWLRQ
,I PRVW RI \RXU DQVZHUV WR WKH SUHYLRXV TXHVWLRQV DUH <HV WKHQ WKH IDFLOLW\ KDV VRPH EDVLF DFFHVVLELOLW\ IHDWXUHV
DQG VKRXOG EH VXUYH\HG XVLQJ WKH $'$ &KHFNOLVW IRU (PHUJHQF\ 6KHOWHUV :KHQHYHU PRVW RI \RXU DQVZHUV DUH
1R WKHQ WKHVH SUREOHPV VKRXOG EH HYDOXDWHG EHIRUH FRQGXFWLQJ D PRUH GHWDLOHG VXUYH\ RU SHUKDSV \RX VKRXOG
FRQVLGHU DQRWKHU ORFDWLRQ WR VHUYH DV DQ HPHUJHQF\ VKHOWHU
Notes/Comments
Yes _____ No _____
Yes _____ No _____
10
Accessible Quick-Check Survey
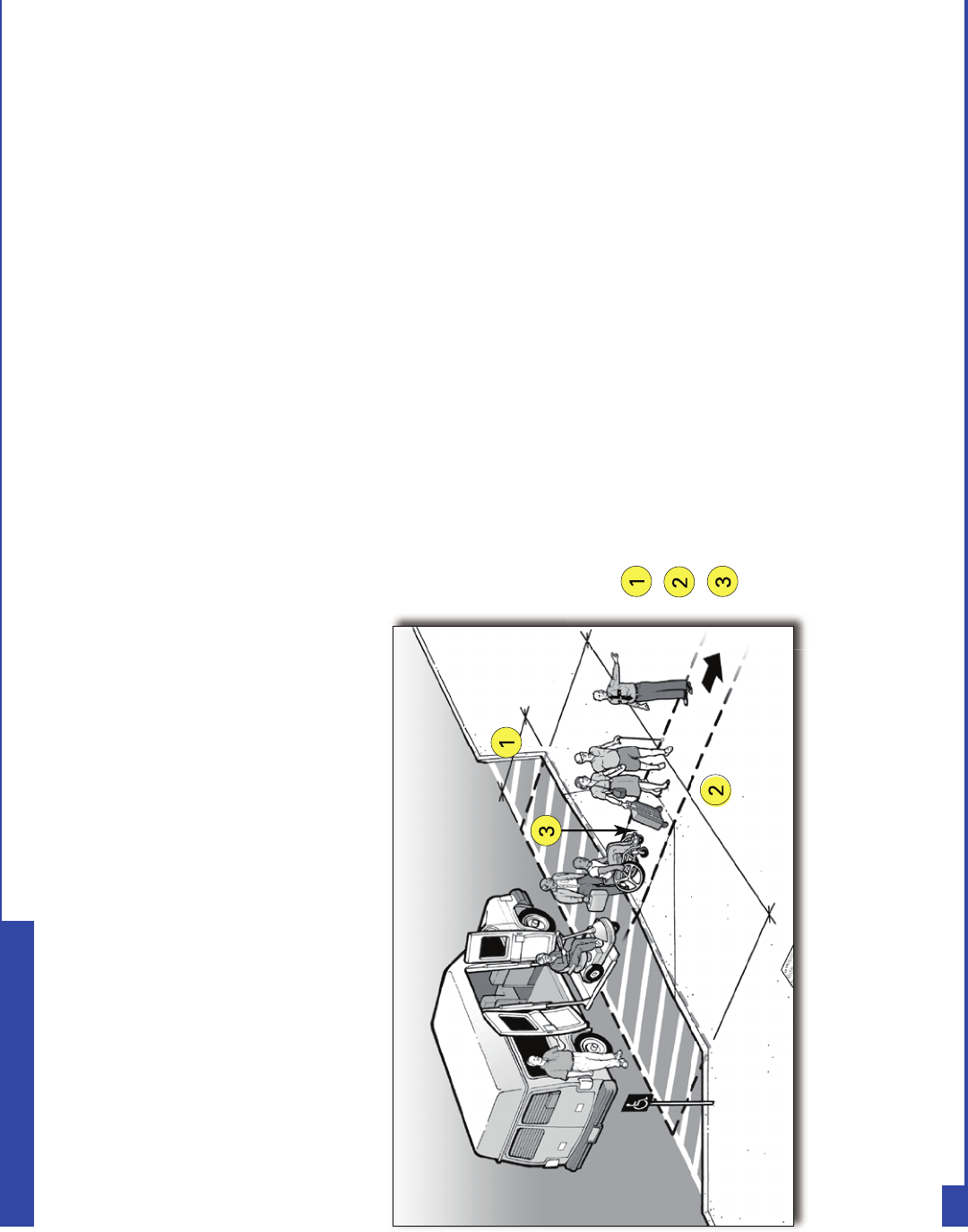
STEP TWO
-
ADA CHECKLIST FOR EMERGENCY SHELTERS
Getting to the Emergency Shelter
A. Passenger Drop-Off Areas
Notes:
Access aisle depth is at least 5 feet.
Access aisle length is at least 20 feet.
Curb ramp connects the access aisle
for the accessible drop- off area
(which is at the level of the parking
lot) to the accessible route to the
accessible entrance of the shelter.
11
ADA Emergency Shelter Checklist
'XULQJ DQ HYDFXDWLRQ WKH PRVW HIÀFLHQW PHWKRG RI WUDQVSRUWLQJ SHRSOH WR VKHOWHUV OLNHO\ ZLOO LQFOXGH XVLQJ YDQV DQG EXVHV $FFHVVLEOH EXVHV
DQG YDQV ZLWK ZKHHOFKDLU OLIWV ZLOO EH QHHGHG WR WUDQVSRUW SHRSOH ZKR XVH ZKHHOFKDLUV VFRRWHUV RU RWKHU PRELOLW\ DLGV :KHQ WKH\ DUULYH DW
WKH VKHOWHU DQ DFFHVVLEOH GURSRII DUHD DOVR NQRZQ DV D SDVVHQJHU ORDGLQJ ]RQH LV QHHGHG IRU SHRSOH XVLQJ PRELOLW\ DLGV WR JHW RII RI WKH EXV
RU YDQ DQG SURFHHG WR WKH VKHOWHU·V DFFHVVLEOH HQWUDQFH
$Q DFFHVVLEOH GURSRII DUHD PXVW KDYH D OHYHO DFFHVV DLVOH WKDW LV
DGMDFHQW DQG SDUDOOHO WR WKH YHKLFOH VSDFH :KHUH D FXUE VHSDUDWHV
WKH YHKLFOH VSDFH IURP WKH DFFHVV DLVOH RU WKH DFFHVV DLVOH IURP
DQ DFFHVVLEOH URXWH D FXUE UDPS PXVW EH SURYLGHG VR SHRSOH ZLWK
PRELOLW\ GLVDELOLWLHV FDQ JHW WR WKH DFFHVVLEOH URXWH OHDGLQJ WR WKH
DFFHVVLEOH HQWUDQFH RI WKH VKHOWHU
Accessible drop-off area with an access aisle provided
at the same level as the vehicle.
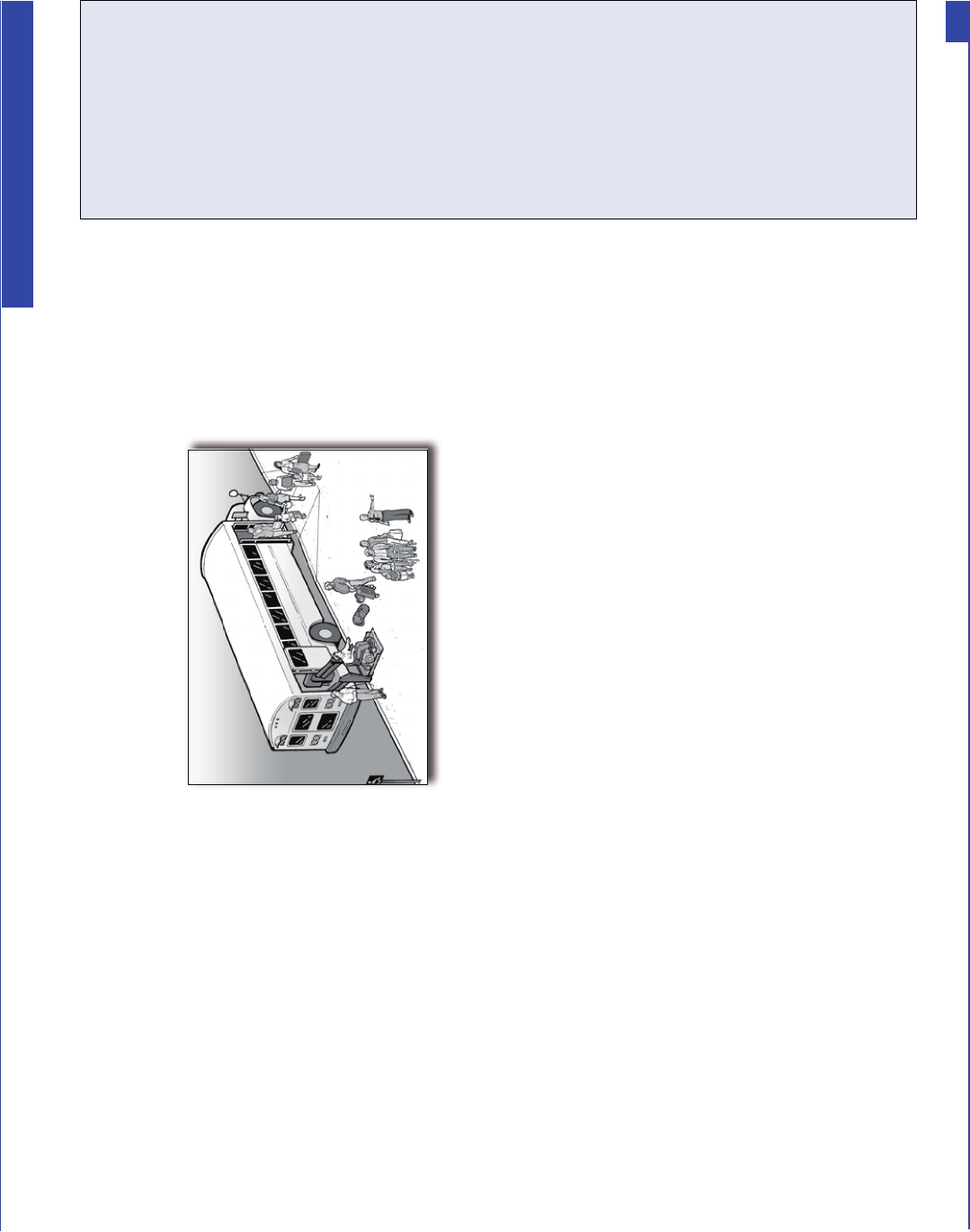
7KH DFFHVV DLVOH PD\ EH DW WKH SDUNLQJORW OHYHO RU DW VLGHZDON OHYHO ,I WKH DFFHVV DLVOH
LV DW WKH SDUNLQJORW OHYHO WKH FXUE UDPS LV SURYLGHG EHWZHHQ WKH DFFHVV DLVOH DQG WKH
VLGHZDON ,I LW LV DW WKH VLGHZDON OHYHO DQ DGMDFHQW FXUE UDPS LV SURYLGHG EHWZHHQ WKH
VWUHHW DQG WKH VLGHZDON
A1. Is a relatively level (1:50 or 2%
maximum slope in all directions)
access aisle provided adjacent
and parallel to the side of the
vehicle pull-up area?
[ADA Standards § 4.6.6]
If No, look for another relatively level
location that is on an accessible route
to the accessible shelter entrance that
could be used.
A2. Is the vehicle pull-up area relatively level (1:50 or 2% maximum slope in
all directions)?
A3. Is the area for the access aisle at least 5-feet wide and 20-feet long?
[ADA Standards § 4.6.6].
Note: Unlike at an accessible parking space, the surface for the access aisle of an
accessible passenger drop-off area does not have to be marked or striped.
A4. Is there vertical clearance of at least 114 inches (9 feet 6 inches) from the
site entrance to the vehicle pull-up area, the access aisle, and along the
vehicle route to the exit? [ADA Standards § 4.6.5]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Accessible drop-off area with an access
aisle provided as part of the sidewalk.
Yes _____ No _____
Notes/Comments
12
ADA Emergency Shelter Checklist
A5. Is a curb ramp provided between the vehicle pull up area and the access
aisle (see above) or the access aisle and the accessible route to the
accessible entrance? [ADA Standards § 4.6.6]
If No, is there another area with a curb ramp and on an accessible route that could
serve as the drop-off area? If there is no curb ramp near the drop-off area, can a
temporary ramp be used to connect the drop-off area access aisle to the accessible
route to the accessible shelter entrance?
A6. If a curb ramp is provided, is the running slope of the ramp surface (not
counting the side flares) no more than 1:12 or 8.33%?
[ADA Standards § 4.7.2]
A7. Is the width of the curb ramp surface at least 36 inches (not counting the
side flares)? [ADA Standards § 4.7.3]
A8. Does an accessible route connect the curb ramp to the shelter’s
accessible entrance? [ADA Standards § 4.1.2(1)]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
13
ADA Emergency Shelter Checklist
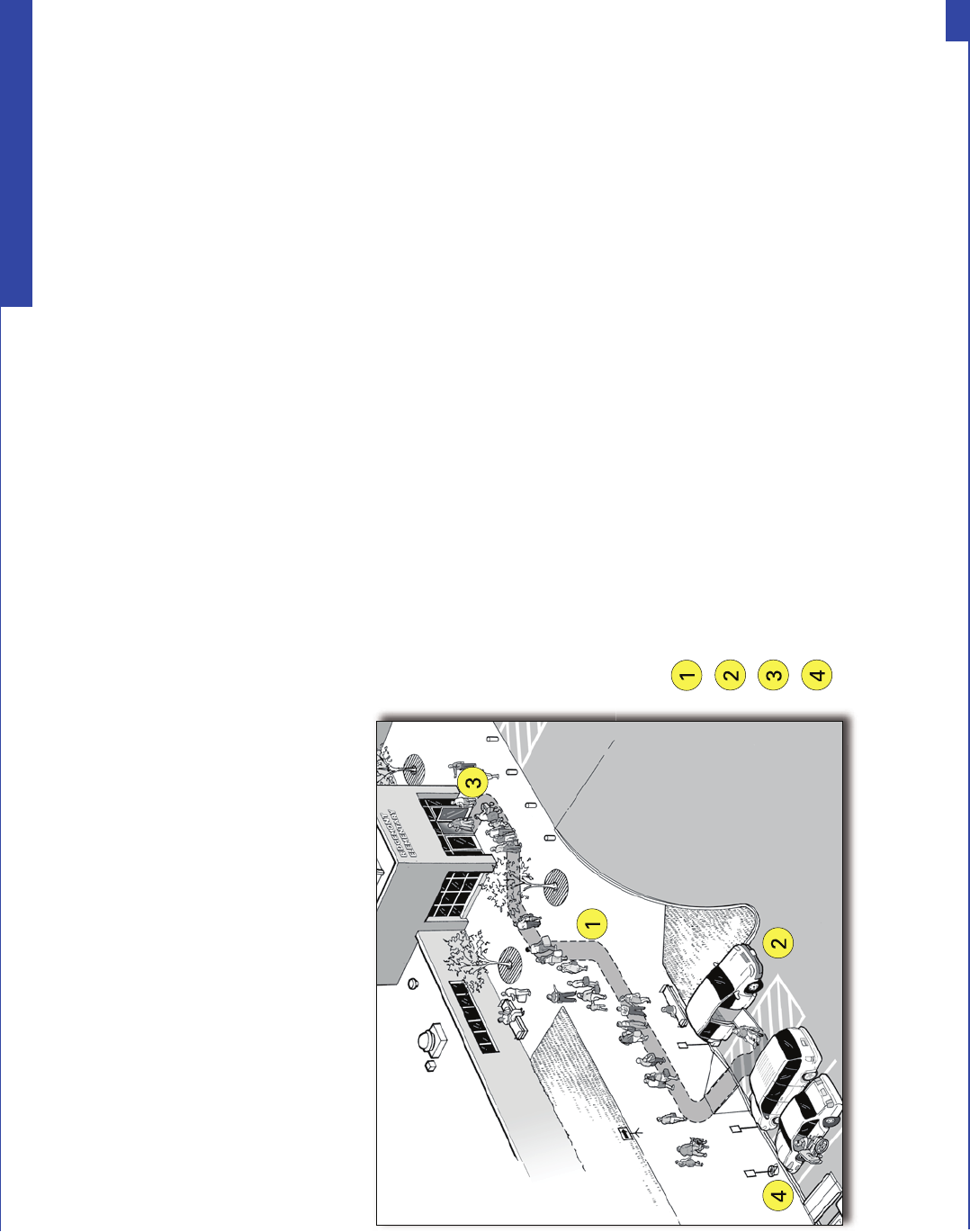
Notes:
Accessible route.
Accessible parking with van accessible parking space.
Accessible entrance to shelter.
Temporary accessible parking spaces.
B. Parking
1. Typical Issues
'XULQJ DQ HYDFXDWLRQ VRPH LQGLYLGXDOV ZLWK D PRELOLW\ GLVDELOLW\ PD\ DUULYH DW WKH VKHOWHU LQ D FDU RU YDQ :KHQ SDUNLQJ DUHDV DUH SURYLGHG
DW WKH VKHOWHU VLWH DFFHVVLEOH SDUNLQJ VSDFHV PXVW EH SURYLGHG ,QGLYLGXDOV ZLWK GLVDELOLWLHV ZKR DUULYH DW WKH VKHOWHU LQ WKHLU RZQ FDU RU YDQ
QHHG WR EH DEOH WR SDUN LQ DQ DFFHVVLEOH SDUNLQJ VSDFH FORVH WR DQ DFFHVVLEOH HQWUDQFH $FFHVVLEOH SDUNLQJ VSDFHV QHHG DQ DGMDFHQW DFFHVV DLVOH
WKDW SURYLGHV VSDFH IRU D SHUVRQ ZLWK D PRELOLW\ GLVDELOLW\ WR H[LW WKHLU YHKLFOH 7KH DFFHVV DLVOH FRQQHFWV GLUHFWO\ WR DQ DFFHVVLEOH URXWH WKDW
OHDGV WR DQ DFFHVVLEOH EXLOGLQJ HQWUDQFH ,Q RUGHU WR EH XVDEOH WKH DFFHVV DLVOH PXVW EH UHODWLYHO\ OHYHO FOHDU RI JUDYHO RU PXG DQG WKH VXUIDFH
PXVW EH LQ JRRG FRQGLWLRQ ZLWKRXW ZLGH FUDFNV RU EURNHQ SDYHPHQW
$Q DFFHVVLEOH URXWH FRQQHFWV WKH SHUPDQHQW DFFHVV DLVOH RI HDFK DFFHVVLEOH
SDUNLQJ VSDFH ZLWK WKH DFFHVVLEOH HQWUDQFH WR WKH VKHOWHU :KHQ DQ DFFHVVLEOH
URXWH FURVVHV D FXUE D FXUE UDPS PXVW EH SURYLGHG 'XULQJ DQ HPHUJHQF\
DV D WHPSRUDU\ PHDVXUH LI DGGLWLRQDO DFFHVVLEOH SDUNLQJ VSDFHV DUH QHHGHG D
SRUWDEOH UDPS FDQ EH SURYLGHG LQ D SDUNLQJ VSDFH PDUNHG RII E\ WUDIÀF FRQHV WR
SURYLGH WZR DGGLWLRQDO DFFHVVLEOH SDUNLQJ VSDFHV VHH SDJH
An access b e entrance to an emergency s e ter
with accessible parking and additional temporary
accessible parking spaces
14
ADA Emergency Shelter Checklist
A il hl
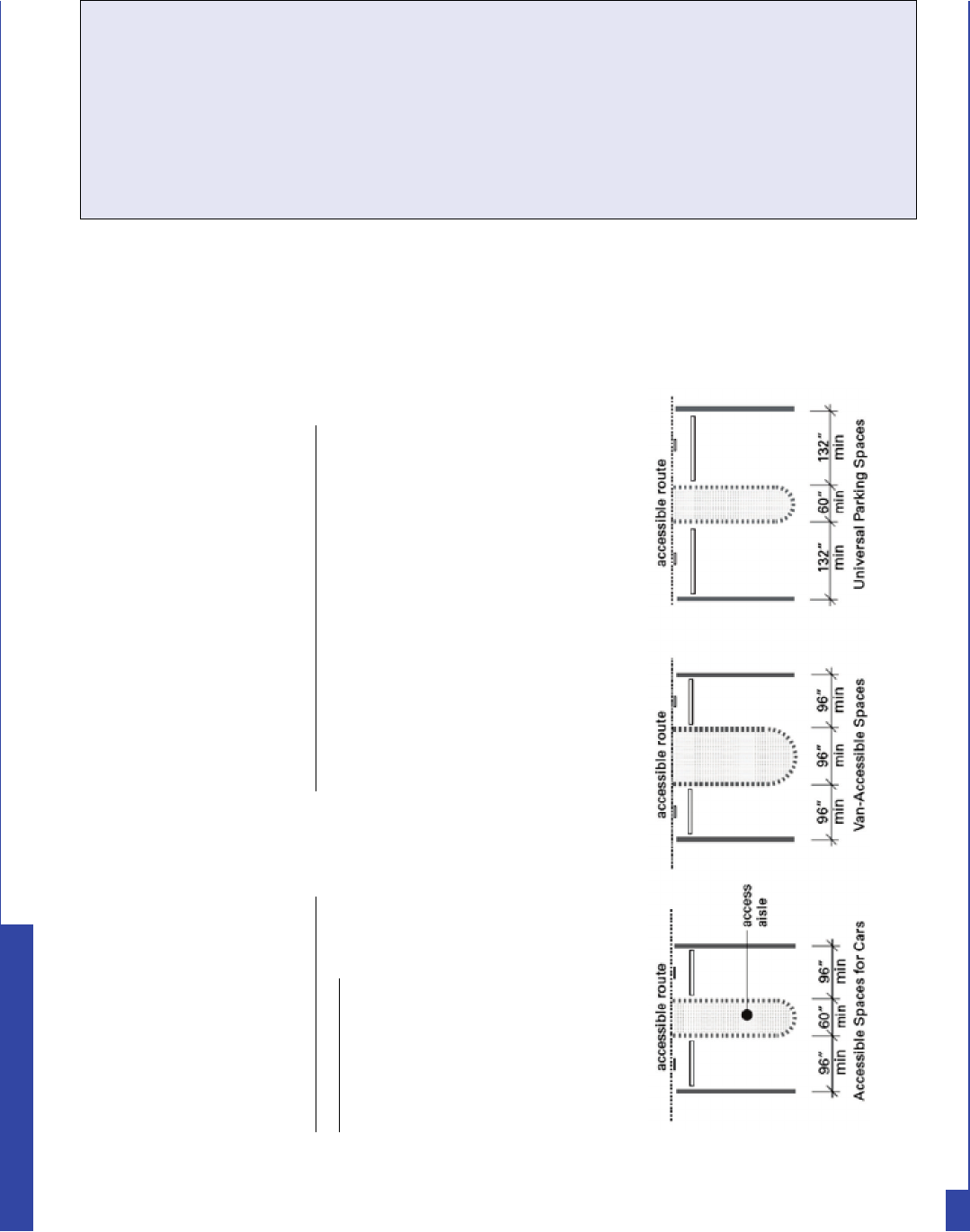
2. Parking Spaces Checklist
B1. When parking areas are provided at the shelter site, count the total
number of parking spaces provided in each area. Is the minimum
number of accessible parking spaces provided, based on the total
number of available parking spaces (see table below)?
[ADA Standards § 4.1.2(5)(a)]
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Accessible Parking Spaces Showing Minimum Width of Vehicle Space and Access Aisle
1 - 25 ..................................................................1 van-accessible space w/min. 96-inch-wide access aisle (van space)
26 - 50 ................................................................1 space w/min. 60-inch-wide access aisle + 1 van space
51 - 75 ................................................................2 spaces w/min. 60-inch-wide access aisle + 1 van space
76 - 100 ..............................................................3 spaces w/min. 60-inch-wide access aisle + 1 van space
101 - 150 .............................................................4 spaces w/min. 60-inch-wide access aisle + 1 van space
If more than 150 parking spaces are provided in a particular lot,
see section 4.1.2 of the ADA Standards for the number of accessible parking spaces required.
Total Number of Parking Spaces
in Each Parking Area
Required Minimum Number of Accessible Spaces
B2. Does each accessible parking space have its own, or share, an adjacent
access aisle that is least 60 inches (5 feet) wide? [ADA Standards § 4.6.3]
15
ADA Emergency Shelter Checklist
B3. Is there at least one van-accessible parking space provided with an
access aisle that is at least 96 inches (8 feet) wide or are universal
parking spaces provided that are 132 inches (11 feet) wide for vehicle
space with a 60-inch (5-feet) wide access aisle?
[ADA Standards § § 4.1.2(5), A4.6]
B4. For van-accessible spaces (particularly in a garage or parking structure),
is there vertical clearance of at least 98 inches (8 feet - 2 inches) for the
vehicle route to the parking space, the parking space, the access aisle,
and along the vehicle route to the exit? [ADA Standards § 4.6.5]
If No: Can the route be cleared by removing or raising low objects, or can each van-
accessible parking space be relocated?
B5. Are all accessible parking spaces, including the access aisle, relatively
level (1:50 or 2%) in all directions? [ADA Standards § 4.6.3]
If No: Look for a nearby area that is relatively level in all directions that could serve as
an accessible parking space with an accessible route to the accessible entrance to the
shelter.
B6. Does each accessible parking space have a sign with the symbol of
accessibility that is visible when a vehicle is parked in the space?
[ADA Standards § 4.6.4]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
16
ADA Emergency Shelter Checklist
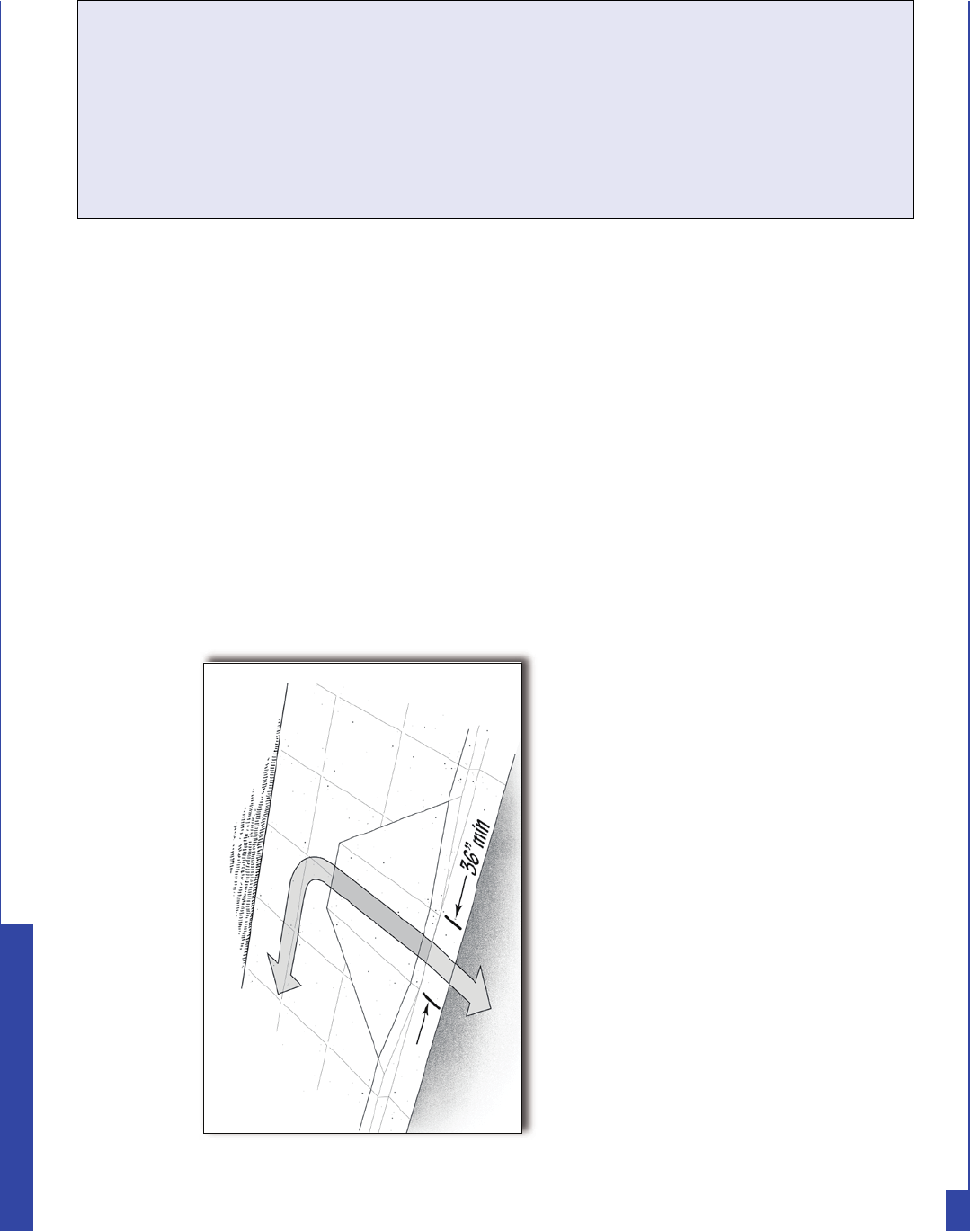
B7. If there is a curb between the access aisle and the accessible route to the
building, is there a curb ramp that meets the following requirements:
[ADA Standards § 4.7]
Yes _____ No _____
Curb ramp showing minimum 36-inch width
for ramp section and 1:12 slope on ramp
section.
Yes _____ No _____
Yes _____ No _____
B7-a. Is the curb ramp surface at least 36 inches wide, excluding flared
sides? [ADA Standards § 4.7.3]
B7-b. Is the slope (up or down the ramp) no more than 1:12?
[ADA Standards § 4.7.2]
Note: 1:12 is one inch of vertical height for each 12 inches of length.
B8. Are the accessible parking spaces serving the shelter on the shortest
accessible route to the accessible entrance? [ADA Standards § 4.6.2]
B9. Does each access aisle connect to an accessible route from the parking
area to the shelter’s accessible entrance? [ADA Standards § 4.6.2]
Yes _____ No _____
Yes _____ No _____
Notes/Comments
17
ADA Emergency Shelter Checklist
6XJJHVWLRQ )LQG D IDLUO\ OHYHO SDUNLQJ DUHD QHDU WKH
DFFHVVLEOH HQWUDQFH DQG PDUN WKH DUHD IRU
DFFHVVLEOH SDUNLQJ VSDFHV 7KUHH UHJXODU
SDUNLQJ VSDFHV ZLOO PDNH WZR DFFHVVLEOH SDUNLQJ
VSDFHV ZLWK D VKDUHG DFFHVV DLVOH 3URYLGH D
VLJQ GHVLJQDWLQJ HDFK DFFHVVLEOH SDUNLQJ VSDFH
(QVXUH WKHUH LV DQ DFFHVVLEOH URXWH IURP HDFK
DFFHVV DLVOH WR WKH DFFHVVLEOH HQWUDQFH
,I WHPSRUDU\ DFFHVVLEOH VSDFHV DUH XVHG PDUN WKH WHPSRUDU\
DFFHVVLEOH SDUNLQJ VSDFHV ZLWK WUDIÀF FRQHV RU RWKHU WHPSRUDU\
HOHPHQWV 7UDIÀF FRQHV FDQ DOVR EH XVHG WR PDUN RII DQ DFFHVV
DLVOH LI GHVLJQDWHG DFFHVVLEOH SDUNLQJ VSDFHV ODFN DQ DFFHVV
DLVOH RU LI WKH DFFHVV DLVOH LV WRR QDUURZ $W OHDVW RQH DFFHVVLEOH
SDUNLQJ VSDFH VKRXOG EH D YDQDFFHVVLEOH SDUNLQJ VSDFH ZLWK DQ
DFFHVV DLVOH WKDW LV DW OHDVW LQFKHV ZLGH
Three standard parking spaces are converted into an accessible
parking space with an access aisle. Cones mark the access aisle
and a temporary curb ramp with edge protection connects to an
accessible route to the shelter.
3. Temporary Solutions for Emergency Sheltering - Parking
3UREOHP 3DUNLQJ DW WKH VKHOWHU IDFLOLW\ HLWKHU KDV QR DFFHVVLEOH
SDUNLQJ QRW HQRXJK DFFHVVLEOH SDUNLQJ RU DFFHVVLEOH
SDUNLQJ VSDFHV DUH QRW RQ OHYHO JURXQG
18
ADA Emergency Shelter Checklist
Notes:
Accessible route
Accessible drop-off area
Accessible parking with van-accessible parking space
Accessible entrance to shelter
C. Sidewalks and Walkways
1. Typical Issues for Individuals Who Use Wheelchairs, Scooters, or other Mobility Devices
$Q DFFHVVLEOH URXWH FRQQHFWV DFFHVVLEOH SDVVHQJHU GURSRII
DUHDV DFFHVVLEOH SDUNLQJ VSDFHV DQG RWKHU DFFHVVLEOH HOHPHQWV
OLNH D URXWH IURP D EXV VWRS WR DQ DFFHVVLEOH EXLOGLQJ HQWUDQFH
7KH DFFHVVLEOH URXWH LV HVVHQWLDO IRU SHRSOH ZKR KDYH GLIÀFXOW\
ZDONLQJ RU ZKR XVH ZKHHOFKDLUV RU RWKHU PRELOLW\ DLGV WR JHW
WR WKH DFFHVVLEOH HQWUDQFH RI WKH VKHOWHU 7KH DFFHVVLEOH URXWH
PXVW EH DW OHDVW LQFKHV ZLGH LW PD\ QDUURZ EULHÁ\ WR
LQFKHV ZLGH ZKHUH XWLOLW\ SROHV VLJQV HWF DUH ORFDWHG DORQJ WKH
DFFHVVLEOH URXWH $EUXSW OHYHO FKDQJHV VWHSV RU VWHHS UXQQLQJ
RU FURVV VORSHV FDQQRW EH SDUW RI DQ DFFHVVLEOH URXWH :KHUH
UDPSV DUH XVHG WKH\ FDQQRW EH VWHHSHU WKDQ 5DPSV ZLWK D
YHUWLFDO ULVH RI PRUH WKDQ LQFKHV PXVW KDYH KDQGUDLOV RQ ERWK
VLGHV 5DPSV PXVW DOVR KDYH HGJH SURWHFWLRQ WR VWRS ZKHHOFKDLUV
IURP IDOOLQJ RII WKH VLGHV DQG OHYHO ODQGLQJV DW WKH WRS DQG
ERWWRP RI HDFK VHJPHQW DQG ZKHUH WKH UDPS FKDQJHV GLUHFWLRQ
An accessible entrance to a shelter with accessible parking
and an accessible drop-off area
19
ADA Emergency Shelter Checklist
C1-a. Is an accessible route provided from accessible parking spaces to the
accessible entrance of the shelter? [ADA Standards § 4.1.2(1), 4.3]
C1-b. Is an accessible route provided from public sidewalks and public
transportation stops on the shelter site (if provided) to the accessible
entrance for the shelter? [ADA Standards § 4.1.2(1)]
Note: The accessible route is at least 36 inches wide and may be a portion of a
sidewalk.
C1-c. Is the accessible route at least 36 inches wide? [ADA Standards § 4.3.3]
If No, does the accessible route narrow to 32 inches for no more than 2 feet?
C1-d. Is the accessible route free of steps and abrupt level changes higher than
1/2 inch? [ADA Standards § 4.3.8]
Note: Level changes between 1/4 inch and 1/2 inch should be beveled (sloped) at 1:2
maximum.
C1-e. Where an accessible route crosses a curb, is a curb ramp provided?
[ADA Standards § 4.3.8]
e-i. Is the curb ramp surface at least 36 inches wide, excluding flared
sides? [ADA Standards § 4.7.3]
e-ii. Is the running slope (up or down the ramp) no more than 1:12?
[ADA Standards § 4.7.2]
Note: 1:12 is one inch of vertical height for 12 inches of horizontal distance.
C1-f. If the slope of part of the accessible route is more than 1:20, does it meet
the following requirements for an accessible ramp?
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
20
ADA Emergency Shelter Checklist
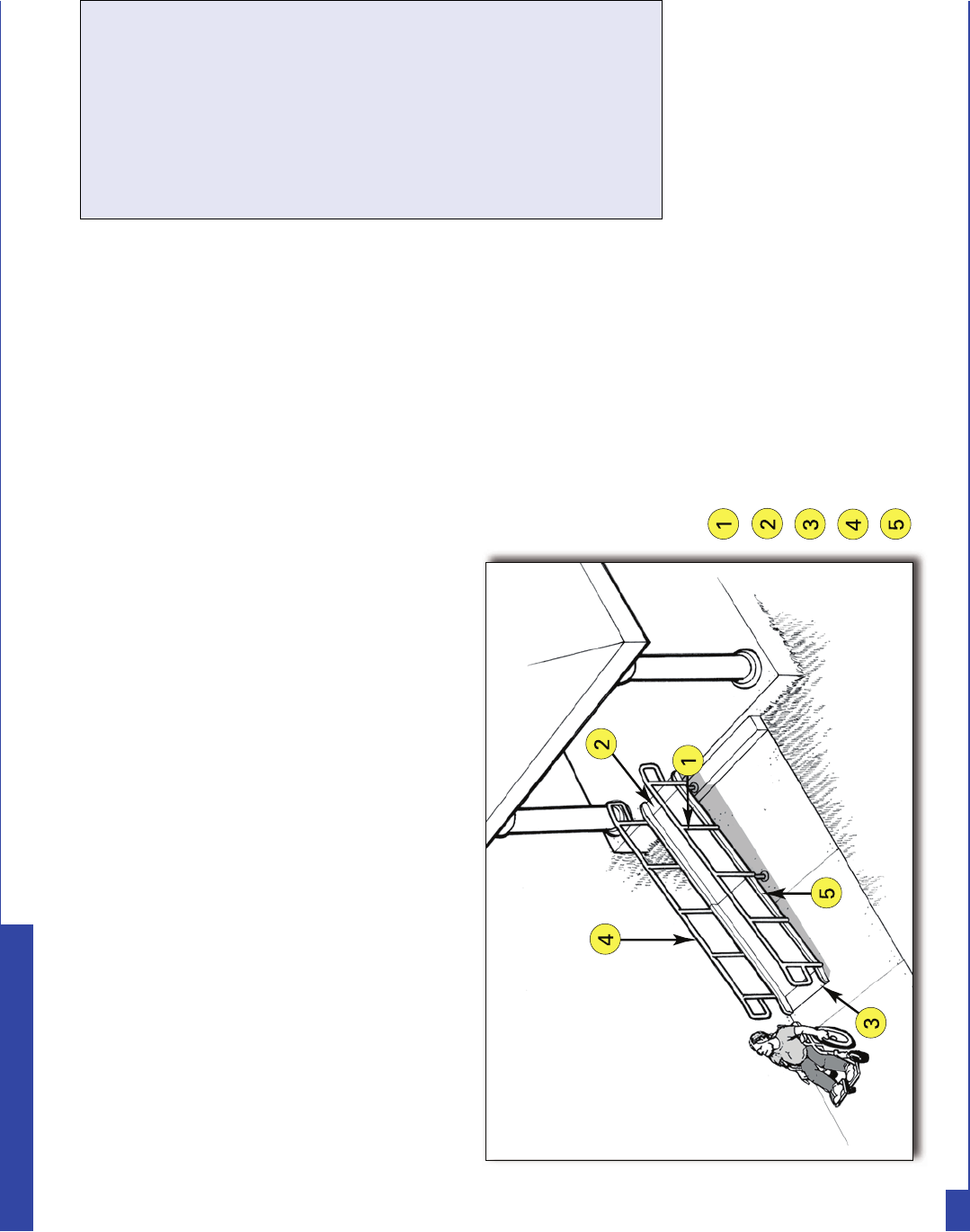
f-i. Is the running slope no greater than 1:12? [ADA Standards § 4.8.2]
Note: For existing ramps, the slope may be 1:10 for a 6-inch rise and 1:8 for
a 3-inch rise in special circumstances (see ADA Standards § 4.1.6(3)).
f-ii. Are handrails installed on both sides of each ramp segment?
[ADA Standards § 4.8.5]
f-iii. Is the ramp width, measured between the handrails, at least 36
inches? [ADA Standards § 4.8.3]
f-iv. Does the ramp have a level landing at the top and bottom of each
ramp section that is at least 60 inches long?
[ADA Standards § 4.8.4]
Note: The level landing may be part of the sidewalk or walking surface.
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
21
ADA Emergency Shelter Checklist
Notes:
At least 36 inches between handrails
Top landing part of walk
Bottom landing part of walk
Handrail height 34 to 38 inches
Edge protection.
Notes/Comments
Temporary Solutions For Emergency Sheltering - Ramps
3UREOHP 7KH VLGHZDON FRQQHFWLQJ SDUNLQJ WR WKH VKHOWHU HQWUDQFH LV WRR VWHHS WR EH DFFHVVLEOH
6XJJHVWLRQ &KHFN WR VHH LI WKHUH LV DQRWKHU DFFHVVLEOH URXWH WR WKH DFFHVVLEOH HQWUDQFH 6RPHWLPHV WKHUH LV D
OHVV GLUHFW URXWH WKDW LV DFFHVVLEOH 'XULQJ DQ HYDFXDWLRQ LW ZLOO EH KHOSIXO WR SXW XS VLJQV RU WR
KDYH YROXQWHHUV VWDWLRQHG DW WKH DFFHVVLEOH SDUNLQJ VSDFHV WR GLUHFW SHRSOH DORQJ WKLV OHVV GLUHFW EXW
QRQHWKHOHVV DFFHVVLEOH URXWH
f-v. If a ramp is more than 30 feet long, is a level landing at least 60
inches long provided at every 30 feet of horizontal length?
[ADA Standards § 4.8.4]
Note: if the running slope is less than 1:16 but more than 1:20, each ramp
segment may be up to 40 feet long followed by a level landing].
f-vi. Is there a level landing, at least 60 inches x 60 inches, when a
ramp changes direction? [ADA Standards § 4.8.4]
f-vii. Are the handrails mounted 34 to 38 inches above the ramp
surface? [ADA Standards § 4.8.5]
f-viii. If the ramp or landing has a vertical drop-off on either side, is
edge protection provided? [ADA Standards § 4.8.7]
Notes/Comments
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
22
ADA Emergency Shelter Checklist
3UREOHP 7KH DFFHVVLEOH URXWH FURVVHV D FXUE EXW QR FXUE UDPS LV
SURYLGHG
6XJJHVWLRQ ,QVWDOO D SRUWDEOH UDPS ZLWK D VORSH QR VWHHSHU WKDQ
ZLWK HGJH SURWHFWLRQ 6WRUH WKH SRUWDEOH UDPS RQ VLWH VR
LW FDQ EH HDVLO\ DFFHVVHG LQ DQ HPHUJHQF\
A portable ramp with edge protection
is installed over a curb to provide an
accessible route.
3UREOHP 7KHUH DUH WZR VWHSV ZKHUH WKH VLGHZDON FRQQHFWV WR WKH
DFFHVVLEOH HQWUDQFH
6XJJHVWLRQ ,QVWDOO D SRUWDEOH UDPS ZLWK D VORSH QR VWHHSHU WKDQ
ZLWK HGJH SURWHFWLRQ DQG KDQGUDLOV RQ ERWK VLGHV RI WKH
UDPS 6WRUH WKH SRUWDEOH UDPS DQG FRPSRQHQWV RQ VLWH
VR HYHU\WKLQJ FDQ EH HDVLO\ DFFHVVHG LQ DQ HPHUJHQF\
A portable ramp with edge protection and handrails is
installed over two steps to provide an accessible route.
23
ADA Emergency Shelter Checklist
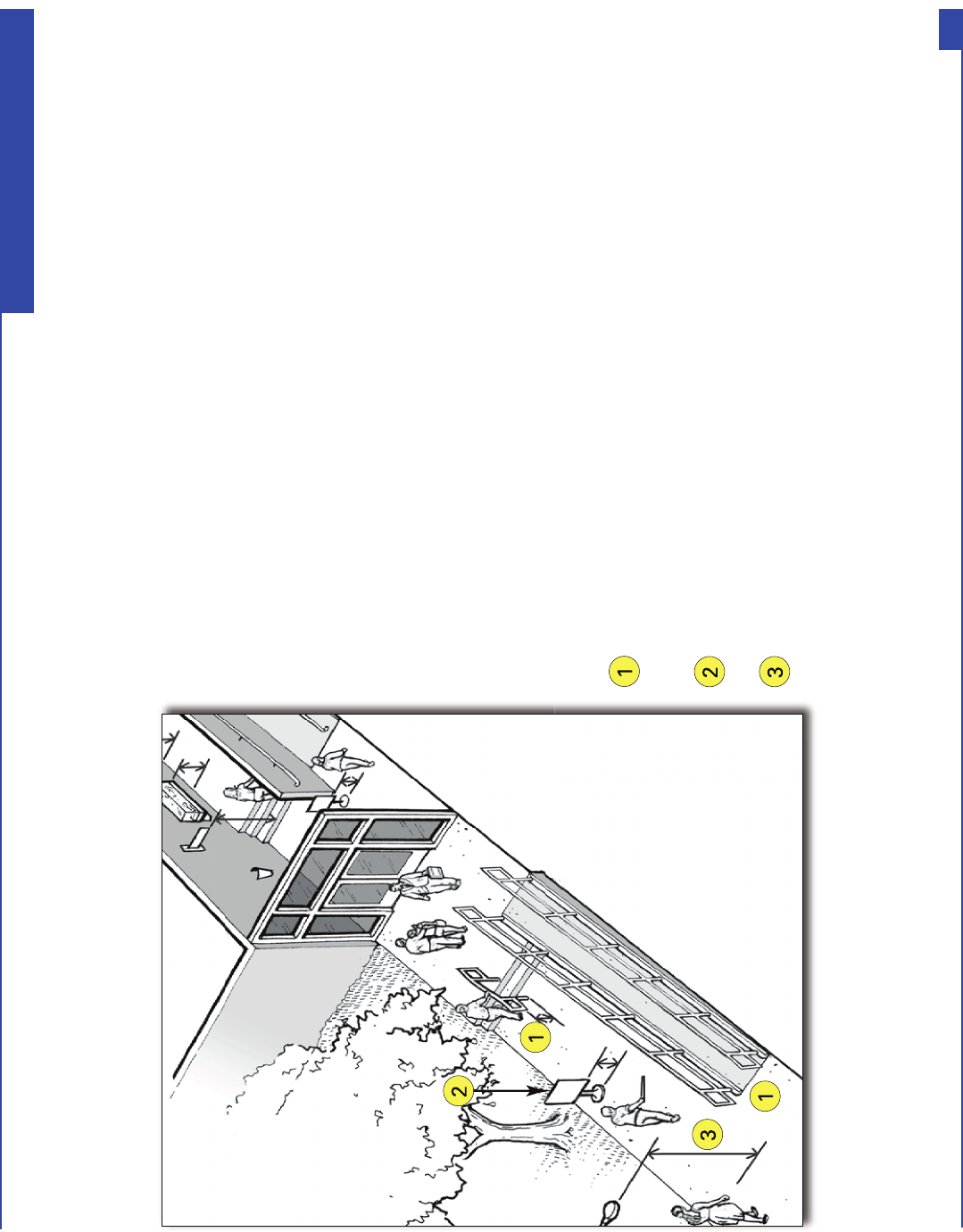
Notes:
The bottom of the handrail extensions turn down to 27 inches
or less above the route so a person who is blind or has low
vision can detect the hazard before running into it.
Signs or other objects in the pedestrian route can be a hazard if the
bottom is more than 27 inches but less than 80 inches above the route.
Objects that overhang the pedestrian route must
be at least 80 inches above the route.
2EMHFWV WKDW DUH ZDOO PRXQWHG WKDW SURMHFW LQWR D SHGHVWULDQ URXWH IURP WKH
VLGH RU WKDW DUH RYHUKHDG FDQ EH KD]DUGV WR SHRSOH ZKR DUH EOLQG RU ZKR KDYH
ORZ YLVLRQ 7KHVH REMHFWV PXVW EH SRVLWLRQHG VR SHRSOH ZLOO HLWKHU GHWHFW WKH
REMHFWV EHIRUH WKH\ UXQ LQWR WKHP RU VDIHO\ SDVV XQGHU WKHP ([DPSOHV PD\
LQFOXGH KDQGUDLO H[WHQVLRQV RQ VWDLUV DQG UDPSV SRVW RU ZDOOPRXQWHG VLJQV
GULQNLQJ IRXQWDLQV DQG ORZ KDQJLQJ WUHH OLPEV 3HGHVWULDQ URXWHV RSHQ WR
SHRSOH GXULQJ WKH WLPH WKDW WKH IDFLOLW\ LV EHLQJ XVHG DV DQ HPHUJHQF\ VKHOWHU
VXFK DV VLGHZDONV FRXUW\DUGV DQG SOD]DV PXVW EH IUHH RI RYHUKDQJLQJ
REMHFWV WKDW DUH OHVV WKDQ LQFKHV DERYH WKH URXWH 2EMHFWV PRUH WKDQ
LQFKHV DQG OHVV WKDQ LQFKHV DERYH WKH URXWH DQG WKDW SURWUXGH IURP WKH VLGH
PRUH WKDQ LQFKHV DUH DOVR D KD]DUG 6LQFH SHRSOH FDQ ZDON RQ DQ\ VLGHZDON
QRW MXVW WKH DFFHVVLEOH URXWHV DOO H[WHULRU SHGHVWULDQ URXWHV VHUYLQJ RU OHDGLQJ
WR WKH VKHOWHU DUHDV PXVW EH FKHFNHG 7KH IROORZLQJ TXHVWLRQV DSSO\ WR
VLGHZDONV DQG ZDONZD\V OHDGLQJ WR WKH HPHUJHQF\ VKHOWHU
Common objects along pedestrian routes to a shelter that
can be hazards to people who are blind or have low vision.
2. Typical Issues for Individuals Who Are Blind or Have Low Vision
24
ADA Emergency Shelter Checklist
C2-1. Are all sidewalks and walkways to the shelter free of any objects
(e.g., wall-mounted boxes, signs, handrail extensions) with bottom
edges that are between 27 inches and 80 inches above the walkway
and that extend more than 4 inches into the sidewalk or walkway?
[ADA Standards §§ 4.4, 4.2.1(3), 4.1.3(2)]
If No, can the object be lowered, removed, or modified or can the route be moved so
that the object can be avoided?
C2-2. Are the undersides of exterior stairs enclosed or protected with a cane-
detectable barrier so that people who are blind or have low vision will
not hit their heads on the underside? [ADA Standards § 4.4.2]
If No, can a barrier or enclosure be added below the stair or can the route be relocated
away from the stair?
When the underside of a stair is open, it is a hazard to
people who are blind or have low vision. Enclosing the
area below the stair or installing a cane-detectable barrier
helps this woman to stop before hitting her head.
Yes _____ No _____
Yes _____ No _____
Notes/Comments
25
ADA Emergency Shelter Checklist
Overhead sign and tree branches are least 80
inches above the walk.
C2-3. Are all objects that hang over
the pedestrian routes at least
80 inches above the route?
[ADA Standards § 4.4.2]
If No, can the objects be removed
or relocated, or can a cane
detectable object be added below
that is at no higher than 27 inches?
Yes _____ No _____
Notes/Comments
Temporary Solutions For Emergency Sheltering - Protruding Object Hazards
3UREOHP 2EMHFWV SURWUXGH WRR IDU IURP WKH VLGH LQWR WKH URXWH FDXVLQJ D KD]DUG IRU SHRSOH ZKR DUH EOLQG RU
ZKR KDYH ORZ YLVLRQ
6XJJHVWLRQ :KHQ SHRSOH ZKR DUH EOLQG RU ZKR KDYH ORZ YLVLRQ XVH D FDQH WR GHWHFW KD]DUGV REMHFWV ORFDWHG
DW LQFKHV RU ORZHU DUH GHWHFWDEOH :KHQ DQ REMHFW LV ORFDWHG KLJKHU WKDQ LQFKHV DERYH WKH
JURXQG LW LV D KD]DUG LI WKH REMHFW SURWUXGHV PRUH WKDQ LQFKHV LQWR WKH FLUFXODWLRQ SDWK 7R PDNH D
SURWUXGLQJ REMHFW FDQH GHWHFWDEOH
3ODFH DQ REMHFW EHORZ RU RQ HLWKHU VLGH RI WKH SURWUXGLQJ REMHFW WKDW LV QRW KLJKHU WKDQ
LQFKHV DERYH WKH JURXQG
,I WKH SURWUXGLQJ REMHFW FDQ EH PRYHG ORZHU WKH REMHFW VR WKDW LWV ERWWRP LV QRW PRUH WKDQ
LQFKHV DERYH WKH JURXQG
3UXQH RU DOWHU WKH SURWUXGLQJ REMHFW VR LW GRHV QRW SURWUXGH DERYH WKH URXWH
26
ADA Emergency Shelter Checklist
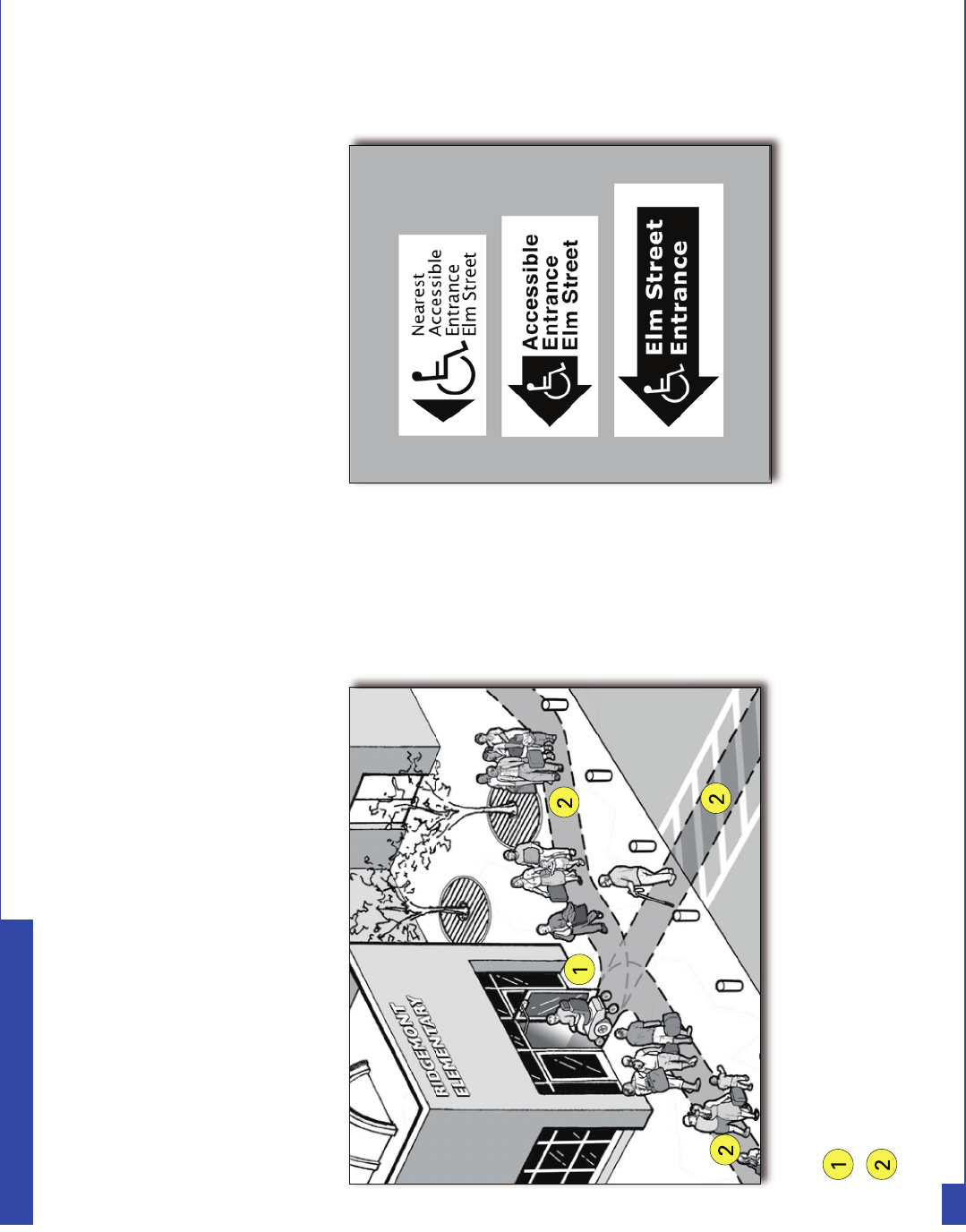
Notes:
Accessible entrance to the shelter.
Accessible route connecting accessible parking and
drop-off area (if provided) to the accessible entrance.
Building Entrance
$ VKHOWHU PXVW KDYH DW OHDVW RQH DFFHVVLEOH HQWUDQFH WKDW LV RQ DQ
DFFHVVLEOH URXWH $Q DFFHVVLEOH HQWUDQFH PXVW SURYLGH DW OHDVW RQH
DFFHVVLEOH GRRU ZLWK PDQHXYHULQJ VSDFH DFFHVVLEOH KDUGZDUH DQG
HQRXJK FOHDU ZLGWK WR DOORZ SHRSOH ZKR XVH FUXWFKHV D FDQH ZDONHU
VFRRWHU RU ZKHHOFKDLU WR XVH LW
D. Entering the Emergency Shelter
Examples of signs for inaccessible
shelter entrances directing people to
the accessible entrance.
,I WKH DFFHVVLEOH HQWUDQFH LV QRW WKH PDLQ HQWUDQFH WR WKH IDFLOLW\
WKDW LV EHLQJ XVHG DV D VKHOWHU VLJQV PXVW EH ORFDWHG DW LQDFFHVVLEOH
HQWUDQFHV WR GLUHFW HYDFXHHV DQG YROXQWHHUV WR WKH DFFHVVLEOH
HQWUDQFH 7KH DFFHVVLEOH HQWUDQFH PXVW EH XQORFNHG ZKHQ RWKHU
VKHOWHU HQWUDQFHV DUH XQORFNHG
27
ADA Emergency Shelter Checklist
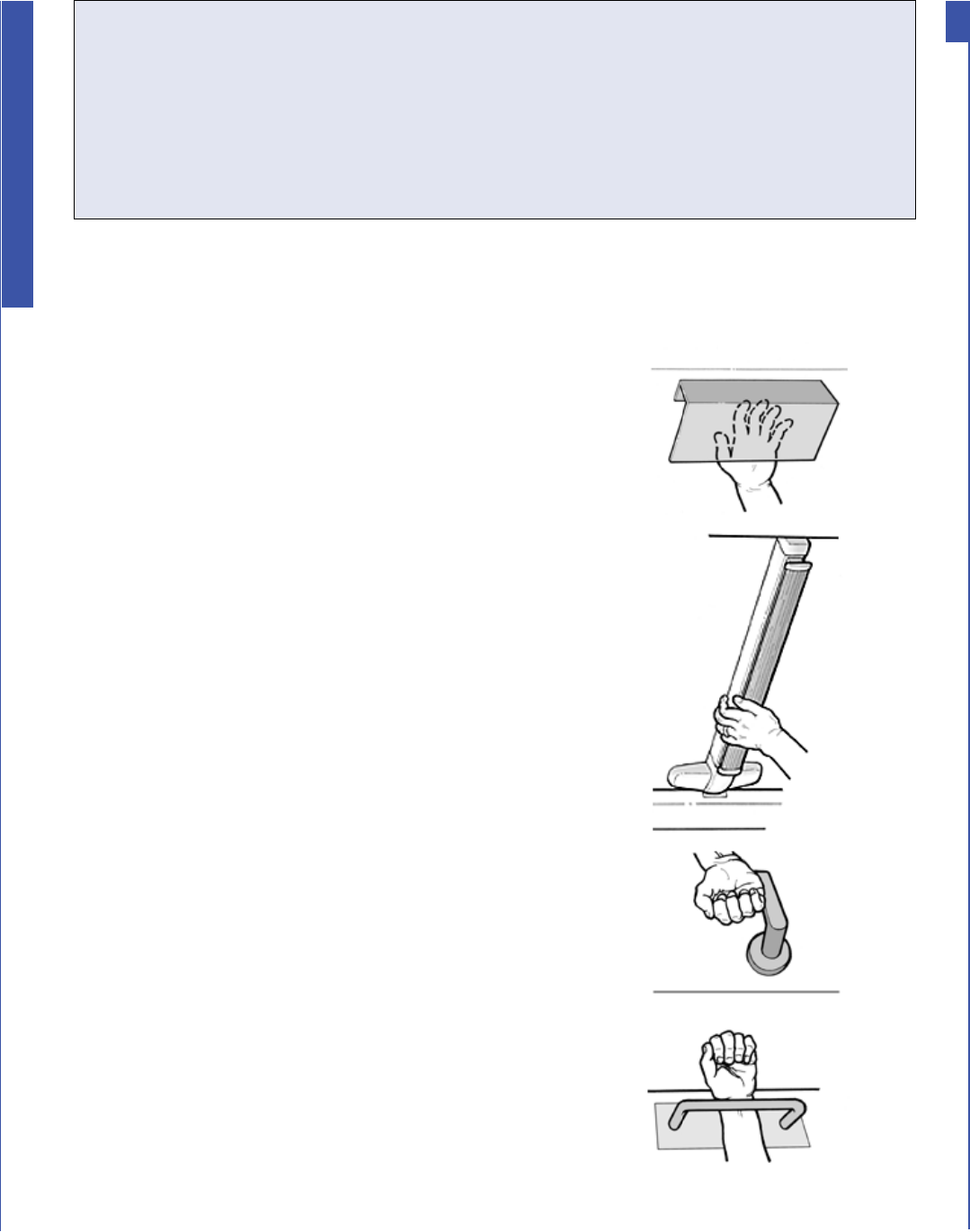
D1. Is there at least one accessible entrance connected to an accessible
route? [ADA Standards § 4.1.3(1)]
Notes: If this entrance is not the main entrance, it needs to be kept unlocked when
other shelter entrances are unlocked.
If there are inaccessible entrances serving the shelter, signs will be needed at
inaccessible entrance(s) to direct evacuees to the nearest accessible entrance.
D2. Does at least one door or one side of a double leaf-door provide at
least 32 inches clear passage width when the door is open 90 degrees?
[ADA Standards § 4.13.5]
If No, does another entrance have an accessible door or can both doors be propped
open during the evacuation? Other possible solutions are to enlarge the door opening,
use a swing clear hinge, or, if a double-leaf door, replace with uneven width doors.
D3. Is the hardware (e.g., lever, pull, and panic bar) usable with one
hand without tight grasping, pinching, or twisting of the wrist?
[ADA Standards § 4.13.9]
If No, leave door propped open, add new accessible hardware, or adapt/replace
hardware.
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
Examples of handles and door hardware that can be used without tight grasping, pinching, or twisting.
28
ADA Emergency Shelter Checklist
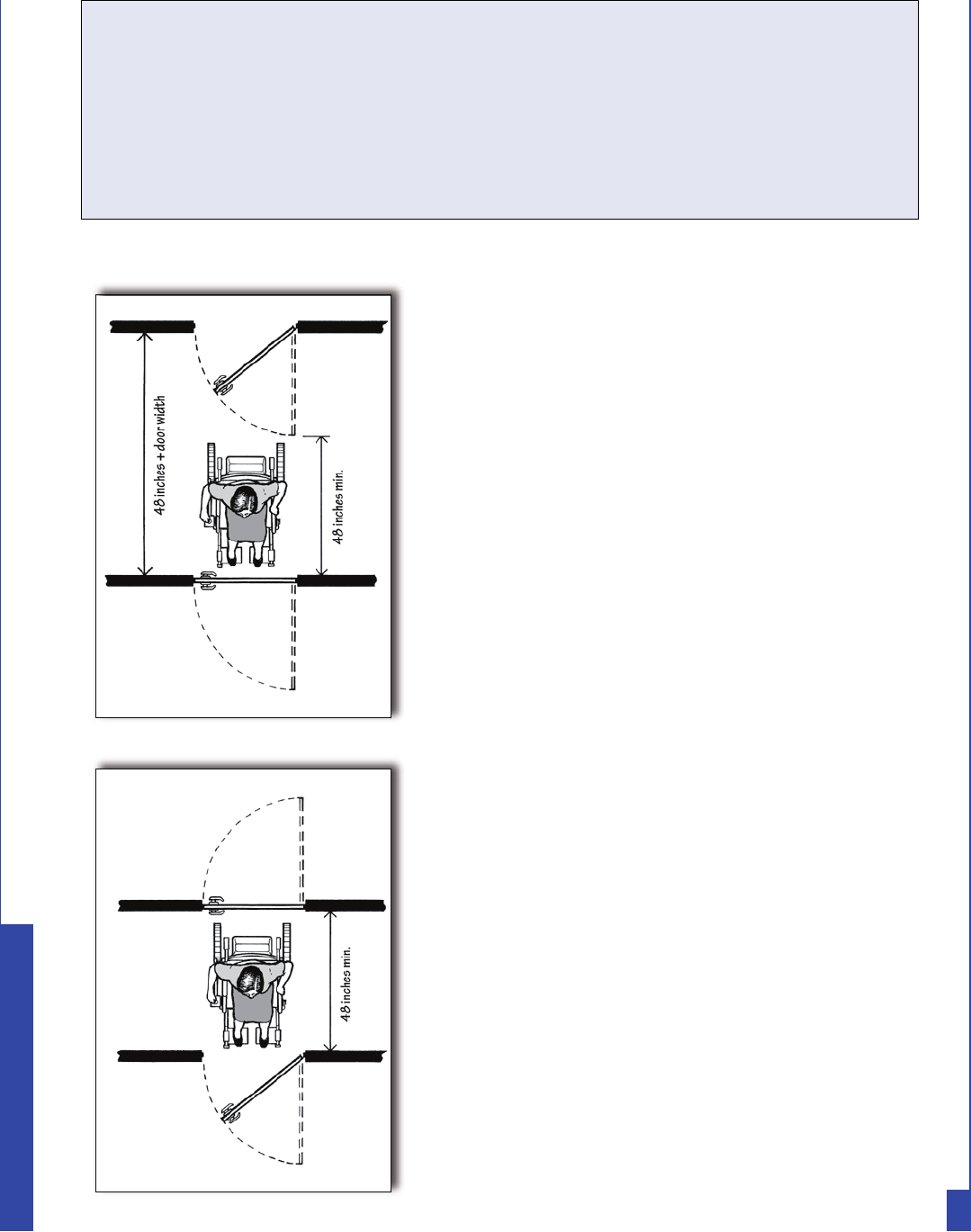
D4. On the latch, pull side of the door, is there at least 18 inches clearance
provided if the door is not automatic or power-operated?
[ADA Standards § 4.13.6, Fig. 25]
If No, leave the door propped open or find another accessible entrance.
D5. If there is a raised threshold, is it no higher than 3/4 inch at the door and
beveled on both sides? [ADA Standards §§ 4.1.6(3)(d)(ii), 4.13.8]
If No, replace threshold with one with beveled sides or add a sloped insert.
D6. If an entry has a vestibule, is there a 30-inch by 48-inch clear floor space
inside the vestibule where a wheelchair or scooter user can be outside
the swing of a hinged door? [ADA Standards § 4.13.7]
If No, leave the inner door permanently open, remove inner door, or modify the
vestibule.
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Minimum vestibule depth of 48 inches if both
doors open out
Minimum vestibule depth of 48 inches + door
width when door swings into vestibule.
Yes _____ No _____
29
ADA Emergency Shelter Checklist
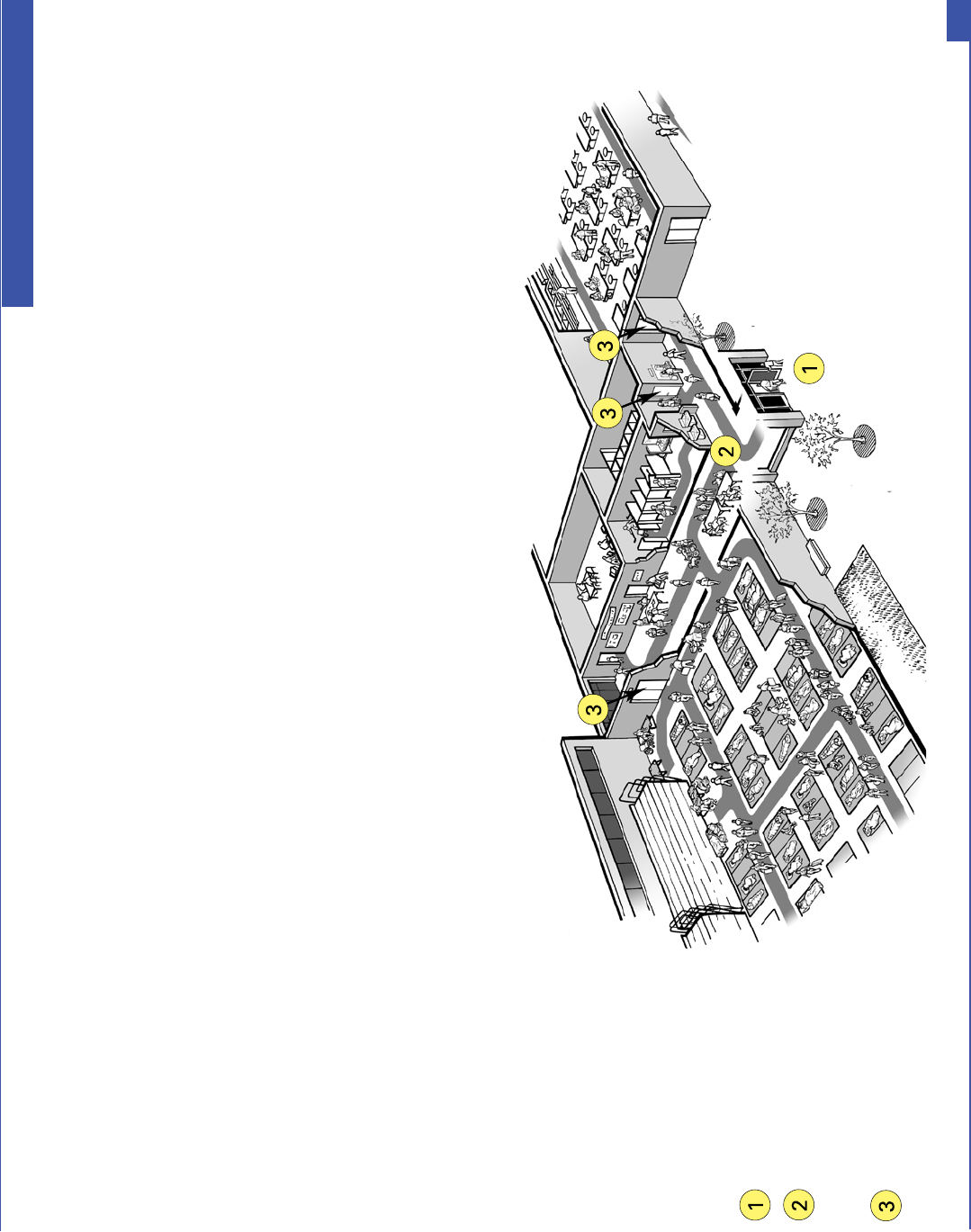
7KH LQWHULRU DFFHVVLEOH URXWH FRQQHFWV WKH DFFHVVLEOH HQWUDQFH ZLWK WKH YDULRXV VHUYLFH DQG DFWLYLW\ DUHDV ZLWKLQ WKH VKHOWHU 7\SLFDOO\ PDGH
XS RI KDOOZD\V FRUULGRUV DQG LQWHULRU URRPV DQG VSDFHV WKH DFFHVVLEOH URXWH LV HVVHQWLDO IRU SHRSOH ZKR KDYH GLIÀFXOW\ ZDONLQJ RU ZKR XVH
ZKHHOFKDLUV RU RWKHU PRELOLW\ DLGV WR JHW WR DOO RI WKH VHUYLFH DQG DFWLYLW\ DUHDV RI WKH VKHOWHU
E. Hallways and Corridors
1. Typical Issues for Individuals Who Use Wheelchairs, Scooters, or Other Mobility Devices
Interior of a shelter showing the accessible route from the
accessible entrance to all service and activity areas.
$Q DFFHVVLEOH URXWH LV DW OHDVW LQFKHV ZLGH DQG PD\ QDUURZ EULHÁ\ WR LQFKHV ZLGH ZKHUH WKH URXWH SDVVHV WKURXJK GRRUV RU QH[W WR
IXUQLWXUH DQG EXLOGLQJ HOHPHQWV +LJK WKUHVKROGV DEUXSW OHYHO FKDQJHV VWHSV RU VWHHS UXQQLQJ RU FURVV VORSHV FDQQRW EH SDUW RI DQ DFFHVVLEOH
URXWH :KHUH UDPSV DUH XVHG WKH\ FDQQRW EH VWHHSHU WKDQ 5DPSV ZLWK D YHUWLFDO ULVH RI PRUH WKDQ LQFKHV PXVW KDYH KDQGUDLOV RQ ERWK
VLGHV 5DPSV PXVW DOVR KDYH HGJH SURWHFWLRQ WR VWRS ZKHHOFKDLUV IURP IDOOLQJ RII WKH VLGHV DQG OHYHO ODQGLQJV DW WKH WRS DQG ERWWRP RI HDFK
VHJPHQW DQG ZKHUH D UDPS FKDQJHV GLUHFWLRQ
:KHUH DQ DFFHVVLEOH URXWH LV GLIIHUHQW IURP WKH URXWH XVHG E\ PRVW HYDFXHHV VLJQV ZLOO
EH QHHGHG DW NH\ GHFLVLRQ SRLQWV WR GLUHFW LQGLYLGXDOV ZLWK GLVDELOLWLHV WR WKH YDULRXV
DFWLYLW\ DUHDV
Notes:
Accessible Entrance
Accessible Route connects the
accessible entrance with shelter
service and activity area
Accessible door to service
and activity areas
30
ADA Emergency Shelter Checklist
E1-a. Is there an accessible route, at least 36 inches wide, that connects the
accessible entrance to all shelter areas (it may narrow to 32 inches wide
for up to 2 feet in length)? [ADA Standards § 4.3.2(3)]
E1-b. Is the accessible route free of steps and abrupt level changes over 1/2
inch?
Note: level changes between 1/4 inch and 1/2 inch should be beveled).
[ADA Standards §§ 4.1.3(1), 4.3.8]
E1-c. Does the accessible route from the accessible entrance to
all activity areas change levels using a ramp, lift or elevator?
[ADA Standards §§ 4.1.3(1), 4.3.8]
If No, go to question E1-g.
c-i. If Yes, is a ramp or sloped hallway provided?
If Yes, go to question E1-d.
c-ii. Is an elevator or lift provided?
If Yes, and the elevator or lift is part of the accessible route to a shelter area, is
back-up electrical power available to operate the elevator or lift for the duration
of shelter operation should the normal electrical service be disrupted?
If Yes and an elevator is provided, see question E1-e.
If Yes and a lift is provided, see question E1-f.
If No, then either provide back-up electrical power to operate the lift or elevator
during the power outage or locate shelter services exclusively on accessible
levels that may be reached by people with a mobility disability without using
an elevator or lift.
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
31
ADA Emergency Shelter Checklist
E1-d. Where the slope of the accessible route is greater than 1:20, does this
area meet the following requirements for an accessible ramp?
d-i. Is the slope no greater than 1:12? [ADA Standards § 4.8.2]
Note: For existing ramps, the slope may be 1:10 for a 6-inch rise and 1:8 for
a 3-inch rise in special circumstances]. [ADA Standards § 4.1.6(3)
d-ii. Are handrails installed on both sides of each ramp segment?
[ADA Standards § 4.8.5]
d-iii. Is the ramp width, measured between handrails, at least 36
inches? [ADA Standards § 4.8.3]
d-iv. Are the handrails mounted 34 to 38 inches above the ramp
surface? [ADA Standards § 4.8.5]
d-v. If a ramp is longer than 30 feet, is a level landing at least 60 inches
long provided every 30 feet? [ADA Standards § 4.8.4]
d-vi. Does the ramp have a level landing that is at least 60 inches long
at the top and bottom of each ramp section or where the ramp
changes direction? [ADA Standards § 4.8.4]
d-vii. If the ramp or landing has a vertical drop-off on either side of the
ramp, is edge protection provided? [ADA Standards § 4.8.7]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
32
ADA Emergency Shelter Checklist
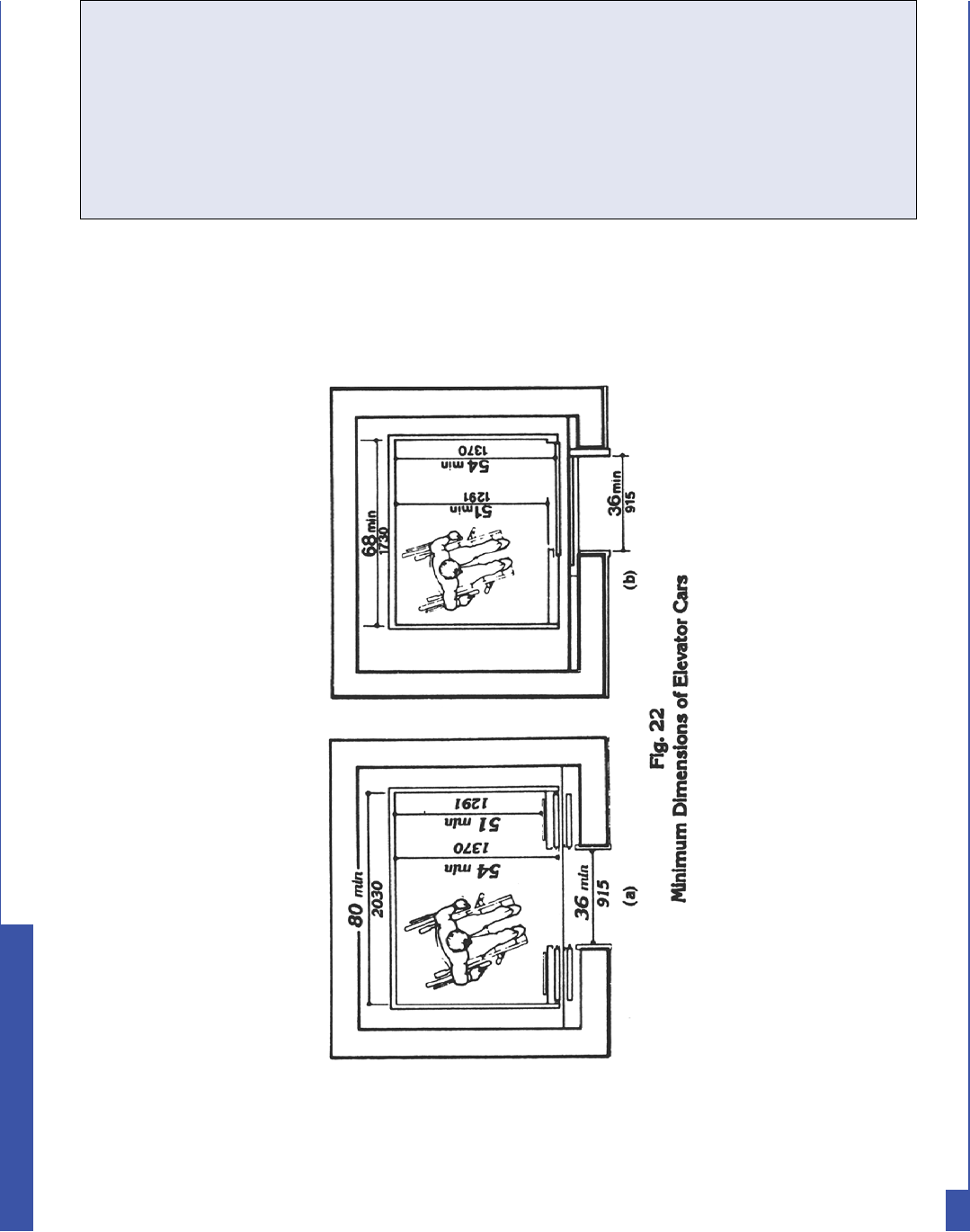
E1-e. Is an elevator provided to each of the levels on which each sheltering
service or activity area is located?
e-i. Are the centerlines of the call buttons mounted 42 inches above
the floor? [ADA Standards § 4.10.3]
e-ii. Does the floor area of the elevator car have space to enter, reach
the controls, and exit? [ADA Standards § 4.10.9, Fig. 22]
e-iii. Can the elevator be called and operated automatically without
using a special key or having to turn on the elevator from a
remote location? [ADA Standards § 4.10.2]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Note: See Figure 22 for acceptable floor and opening dimensions. Floor dimensions of at least
48 inches by 48 inches may be allowed in existing facilities built before the ADA went into effect.
Notes/Comments
Yes _____ No _____
33
ADA Emergency Shelter Checklist
e-iv. Are the highest floor control buttons mounted no more than 54
inches above the floor for a side reach or 48 inches for forward
reach? [ADA Standards § 4.10.12 (3)]
e-v. Are raised letters and Braille characters used to identify each floor
button and each control? [ADA Standards § 4.10.12]
e-vi. Are signs mounted on both sides of the elevator hoistway door
opening (for each elevator and at each floor) that designate
the floor with 2-inch minimum-height raised letters and Braille
characters centered at 60 inches above the floor?
[ADA Standards § 4.10.5]
e-vii. Is the elevator equipped with audible tones or bells or verbal
annunciators that announce each floor as it is passed?
[ADA Standards § 4.10.13]
E1-f. If a wheelchair lift is provided, does it meet the following?
f-i. Is the lift operational at the time of the survey?
[ADA Standards § 4.11.3]
f-ii. Is the change in level from the floor to the lift surface ramped or
beveled? [ADA Standards §§ 4.11.2, 4.5.2]
f-iii. Is there at least a 30-inch by 48-inch clear floor space on the
wheelchair lift? [ADA Standards §§ 4.11.2, 4.2.4]
f-iv. Does the lift allow a person using a mobility device unassisted
entry, operation (is key available, if required), and exit?
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
34
ADA Emergency Shelter Checklist
f-v. Are the controls and operating mechanisms mounted no more
than 54 inches above the floor for a side reach or 48 inches for a
forward reach? [ADA Standards §§ 4.11.2, 4.27.3]
f-vi. Are the controls and operating mechanisms usable with
one hand without tight grasping, pinching, or twisting?
[ADA Standards §§ 4.11.2, 4.27.4]
E1-g. At each location on the way to each shelter activity area where the
accessible route passes through a door, does at least one door meet the
following requirements?
g-i. Is the clear width for the door opening at least 32
inches measured when the door is open 90 degrees?
[ADA Standards §§ 4.1.3(7), 4.13.5]
g-ii. Is the door hardware (e.g., lever, pull, push, panic bar)
usable with one hand, without tight grasping, pinching, or
twisting of the wrist, to allow people who may not be able to
easily use one or both hands to fully operate the hardware?
[ADA Standards § 4.13.9]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
35
ADA Emergency Shelter Checklist

A clear floor space on the latch side of the door (pull side) allows a person using a
wheelchair or scooter to pull the door open and then enter. The size of the clear floor space
varies depending on the direction of approach (shown by the arrows) and the door swing.
g-iii. Is there clear maneuvering floor space in front of each accessible
door (see ADA Standards § Fig. 25) and, on the pull side, is there
at least 18 inches clear floor space beyond the latch side of the
door (see space configurations in Figure 25)?
[ADA Standards § 4.13.6]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
g-iv. Is no more than 5 pounds force needed to push or pull open the
door? [ADA Standards § 4.13.11 (2)(b)]
Note: Fire doors are still considered to be accessible if they have the
minimum opening force allowable by the appropriate administrative
authority.
g-v. If the answers to questions g-ii thru g-iv are No, can the door be
propped open?
If an activity area is not on an accessible route and cannot be made accessible, find another
area that is on an accessible route where that activity may be provided.
36
ADA Emergency Shelter Checklist
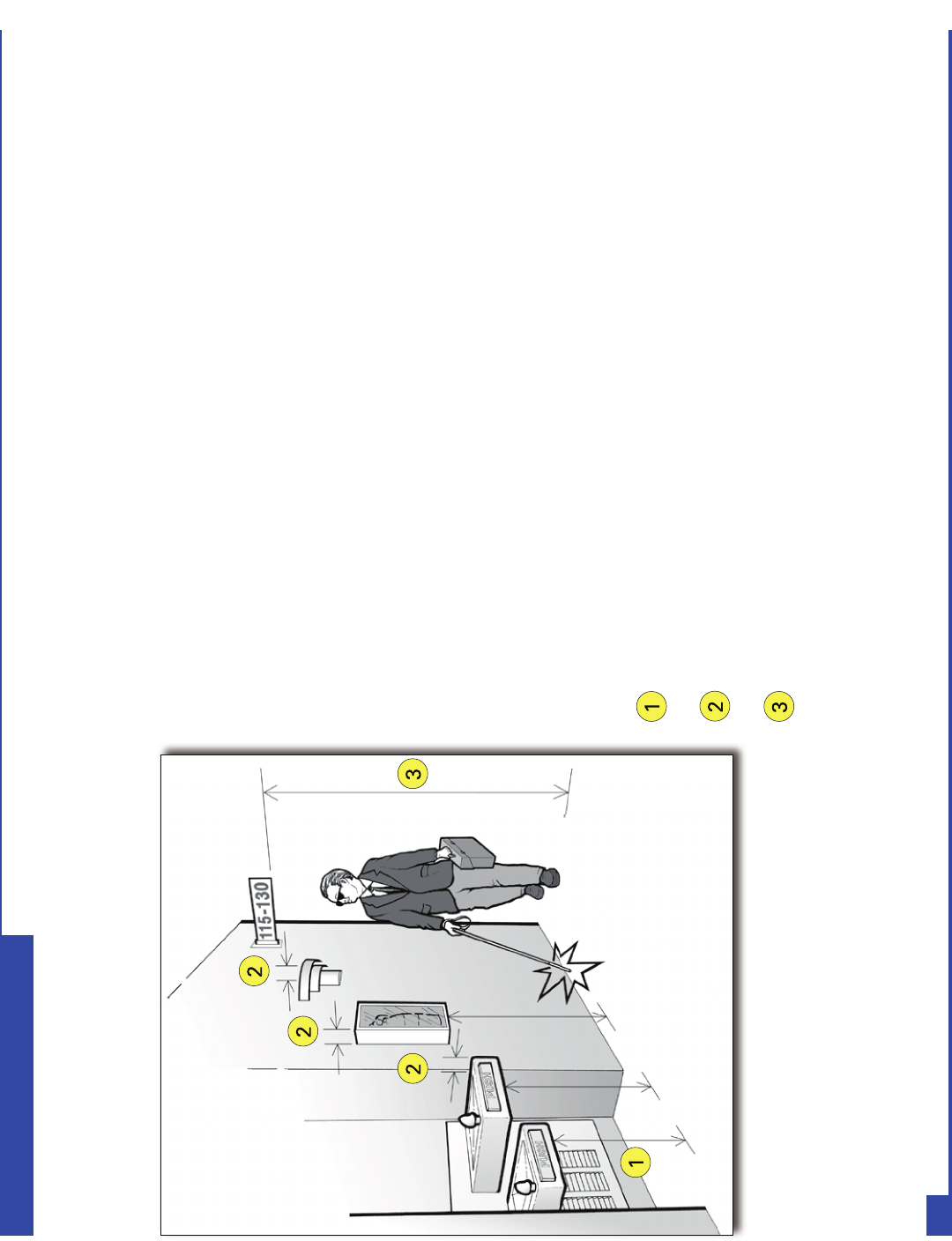
,QGLYLGXDOV ZKR DUH EOLQG RU KDYH ORZ YLVLRQ PD\ ZDON DORQJ DQ\ URXWH RU WKURXJK
DQ\ VKHOWHU DFWLYLW\ DUHD QRW MXVW WKH DFFHVVLEOH URXWHV 7KDW PHDQV DQ\ DUHD
ZKHUH SHRSOH XVLQJ WKH VKHOWHU FDQ ZDON LQFOXGLQJ KDOOZD\V FRUULGRUV HDWLQJ
DUHDV DQG VOHHSLQJ DUHDV PXVW EH IUHH RI REMHFWV WKDW FDQQRW EH GHWHFWHG E\ D
SHUVRQ ZKR LV EOLQG RU KDV ORZ YLVLRQ 2EMHFWV WKDW DUH ZDOO PRXQWHG WKDW SURMHFW
LQWR D SHGHVWULDQ URXWH IURP WKH VLGH RU WKDW DUH RYHUKHDG PXVW EH ORFDWHG VR
WKDW LQGLYLGXDOV ZKR DUH EOLQG RU KDYH ORZ YLVLRQ ZLOO HLWKHU GHWHFW WKH REMHFWV
EHIRUH WKH\ UXQ LQWR WKHP RU VDIHO\ SDVV XQGHU WKHP 7KHVH URXWHV PXVW EH IUHH RI
RYHUKDQJLQJ REMHFWV WKDW DUH OHVV WKDQ LQFKHV DERYH WKH ÁRRU DQG VLGH REMHFWV
WKDW SURWUXGH LQWR WKH URXWH PRUH WKDQ LQFKHV ZKHQ WKH ERWWRP RI WKH REMHFW LV
PRUH WKDQ LQFKHV DERYH WKH ÁRRU ,WHPV WR ZDWFK IRU LQFOXGH ZDOOPRXQWHG ÀUH
H[WLQJXLVKHUV DQG ZDOOPRXQWHG GLVSOD\ FDVHV ZKHQ WKH ERWWRP LV PRUH WKDQ
LQFKHV DERYH WKH ÁRRU ZDOO VFRQFHV DQG OLJKW À[WXUHV WKDW SURWUXGH PRUH WKDQ
LQFKHV RII WKH ZDOO DQG RSHQ VWDLUFDVHV H[LW VLJQV RYHUKHDG VLJQV EDQQHUV DQG
DUFKHG GRRUZD\V WKDW DUH ORZHU WKDQ LQFKHV DERYH WKH ÁRRU
2. Typical Issues for People Who are Blind or Have Low Vision
Notes:
Wall-mounted drinking fountains are a hazard when the front projects more than
4 inches beyond the wall and the bottom is more than 27 inches above the floor.
Wall-mounted objects cannot project more than 4 inches beyond the wall
if
t
he bottom is not in the cane-detectable area below 27 inches off the floor.
Overhead objects must be at least 80 inches off the floor.
Overhead and wall-mounted objects that may be
hazards along a pedestrian route
37
ADA Emergency Shelter Checklist
7KH IROORZLQJ TXHVWLRQV DSSO\ WR SHGHVWULDQ URXWHV VHUYLQJ RU OHDGLQJ WR WKH VKHOWHU DFWLYLW\ DQG FRPPRQ XVH
DUHDV
E2-a. Are pedestrian routes leading to or serving each service or activity area of
the shelter free of objects that protrude from the side more than 4 inches
into the route with the bottom of the object more than 27 inches above
the floor? [ADA Standards § 4.4.1]
Note: These objects may be wall mounted or free standing. Items to check include
wall-mounted fire extinguishers, light fixtures, coat hooks, shelves, drinking
fountains, and display cases.
E2-b. Are pedestrian routes leading to or serving each of the service or activity
areas free of overhead objects with the bottom edge lower than 80
inches above the floor? [ADA Standards § 4.4.2]
E2-c. Are any interior stairs along these
routes configured with a cane-detectable
warning or a barrier that prevents travel
into the area with less than an 80-inch
high head clearance so that people who
are blind or who have low vision cannot
hit their heads on the underside or stair
frame? [ADA Standards § 4.4.2]
If No, list the objects that are a hazard and their
location. Remove or relocate the object or place a
detectable object on the floor below each object to
remove the hazard.
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
38
ADA Emergency Shelter Checklist
When the underside of a stair is open,
it is a hazard to people who are blind
or have low vision. Enclosing the area
below the stair or installing a cane-
detectable barrier helps the person to
avoid the area.
F1. Is there an accessible route that connects the accessible entrance to
areas that are likely to be used to register people as they arrive at the
shelter? [ADA Standards § 4.3]
F2. If there is a built-in reception or other type of counter, does it have a
section that is at least three feet long that is no higher than 36 inches
above the floor or is there a nearby surface that is not higher than 36
inches above the floor? [ADA Standards § 7.2]
Yes _____ No _____
Yes _____ No _____
Notes/Comments
39
ADA Emergency Shelter Checklist
F. Check-In Areas
$ VKHOWHU XVXDOO\ KDV RQH RU PRUH FKHFNLQ DUHDV
ORFDWHG QHDU WKH HQWUDQFH WR WKH VKHOWHU :KHQ
FKHFNLQ DUHDV DUH SURYLGHG WKHQ DW OHDVW RQH
DFFHVVLEOH FKHFNLQ ORFDWLRQ VKRXOG EH SURYLGHG
7KH DFFHVVLEOH FKHFNLQ DUHD VKRXOG EH DW WKH
DFFHVVLEOH HQWUDQFH RU VLJQV VKRXOG JLYH GLUHFWLRQV
WR WKH DFFHVVLEOH FKHFNLQ DUHD
,I D SHUPDQHQW UHFHSWLRQ FRXQWHU LV XVHG IRU FKHFN
LQ PDNH VXUH WR SURYLGH D ZULWLQJ VXUIDFH DW DQ
DFFHVVLEOH KHLJKW IRU SHRSOH ZKR XVH D ZKHHOFKDLU
VFRRWHU RU RWKHU PRELOLW\ GHYLFH 7KLV PD\ EH D
SDUW RI WKH UHFHSWLRQ FRXQWHU WKDW LV QR KLJKHU WKDQ
LQFKHV DERYH WKH ÁRRU D IROGLQJ VKHOI RU DQ
DGMDFHQW WDEOH RU D FOLS ERDUG
An accessible check-in location using a folding table with a
height that people who use wheelchairs can easily reach.
G. Sleeping Areas
(DFK DFFHVVLEOH VOHHSLQJ DUHD QHHGV WR
EH RQ DQ DFFHVVLEOH URXWH FRQQHFWLQJ LW WR
RWKHU DFWLYLW\ DUHDV LQ WKH VKHOWHU LQFOXGLQJ
WRLOHW URRPV DQG EDWKLQJ DUHDV $Q
DFFHVVLEOH URXWH ZLWK DGHTXDWH FLUFXODWLRQ
DQG PDQHXYHULQJ VSDFH SURYLGHV DFFHVV
LQ WKH VOHHSLQJ DUHDV IRU SHRSOH ZKR XVH
ZKHHOFKDLUV RU VFRRWHUV DQG WKLV URXWH VHUYHV
HDFK DFFHVVLEOH EHG RU FRW
Interior of one section of a shelter’s sleeping
area. The shaded pathway indicates the
accessible route, which provides access to
accessible beds, cots, and other activity areas
in the space plus the toilet rooms and other
activity areas in the shelter.
40
ADA Emergency Shelter Checklist
Living at the Emergency Shelter
$FFHVVLEOH FRWV KDYH D VOHHSLQJ VXUIDFH DW
DSSUR[LPDWHO\ WKH VDPH KHLJKW DERYH WKH ÀRRU DV
WKH VHDW RI D ZKHHOFKDLU WR LQFKHV DERYH
WKH ÀRRU :KHQ SODFHG LQ VHYHUDO VHFWLRQV RI WKH
VOHHSLQJ DUHD LQGLYLGXDOV ZKR XVH D ZKHHOFKDLU
VFRRWHU RU RWKHU PRELOLW\ GHYLFH ZLOO EH DEOH WR
VOHHS QHDU WKHLU IDPLO\ RU RWKHU FRPSDQLRQV $Q
DFFHVVLEOH URXWH LV QHHGHG WR SURYLGH DFFHVV WR
HDFK DFFHVVLEOH FRW DQG D FOHDU VSDFH DW OHDVW
LQFKHV ZLGH LV QHHGHG DORQJ WKH VLGH RI WKH FRW WR
PDNH LW SRVVLEOH WR WUDQVIHU EHWZHHQ WKH PRELOLW\
GHYLFH DQG WKH FRW $ SUHIHUUHG ORFDWLRQ IRU
DFFHVVLEOH FRWV LV WR KDYH RQH VLGH DJDLQVW D ZDOO
7KLV KHOSV WR VWDELOL]H WKH FRW DQG WKH ZDOO FDQ DFW
DV D EDFNUHVW ZKHQ WKH SHUVRQ VLWV XS RQ WKH FRW
An accessible cot positioned against a wall. Dashed
lines indicate the accessible route and clear floor
space next to the cot.
G1. Is there an accessible route, at least 36 inches wide, that connects each
sleeping area with other shelter activity areas?
Note: it may narrow to 32 inches wide for up to 2 feet in length.
[ADA Standards § 4.3.2(3)]
G2. Is the accessible route free of steps and abrupt level changes over 1/2 inch?
Note: level changes between 1/4 inch and 1/2 inch should be beveled.
[ADA Standards §§ 4.1.3(1), 4.3.8]
Note: Although the facility survey cannot check the accessibility of the cots
because they will not be installed until the shelter is in use, planning for setting up
the sleeping area and for arranging the cots and mats should include providing
space for an accessible route and clear floor space at each accessible cot. Cots
used by people who are blind or who have low vision should be in an easily
locatable area.
Yes _____ No _____
Yes _____ No _____
Notes/Comments
41
ADA Emergency Shelter Checklist
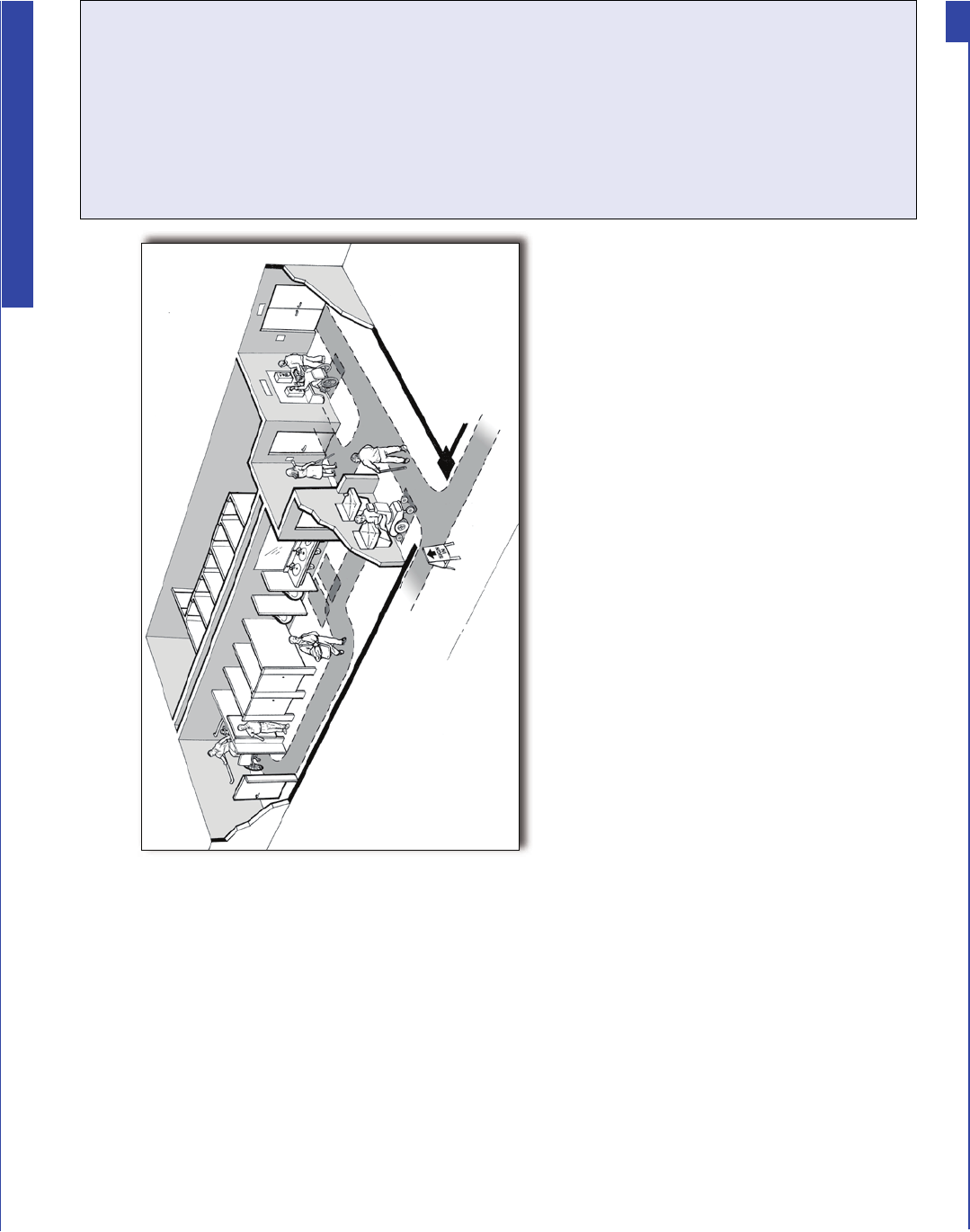
H. Restrooms and Showers
$W OHDVW RQH VHW RI WRLOHW URRPV VHUYLQJ
WKH VKHOWHU PXVW EH DFFHVVLEOH WR
LQGLYLGXDOV ZKR XVH D ZKHHOFKDLU
VFRRWHU RU RWKHU PRELOLW\ GHYLFH ,Q
ODUJH VKHOWHUV ZKHUH PRUH WKDQ RQH
VHW RI WRLOHW URRPV LV QHHGHG WR VHUYH
WKH RFFXSDQWV LW PD\ EH QHFHVVDU\ WR
SURYLGH DGGLWLRQDO DFFHVVLEOH WRLOHW
IDFLOLWLHV RU WR HVWDEOLVK SROLFLHV WR
DVVXUH WKDW LQGLYLGXDOV ZLWK GLVDELOLWLHV
KDYH DFFHVV WR WKH DFFHVVLEOH IDFLOLWLHV
Interior of an accessible toilet room showing accessible route, clear
floor space at accessible fixtures, and the wide accessible toilet stall.
H1. If a sign is provided at the toilet room entrance (e.g. Men, Women, Boys,
Girls, etc.), is a sign with raised characters and Braille mounted on the
wall adjacent to the latch? [ADA Standards § 4.30.6]
If No, install a sign with raised characters and Braille on the wall adjacent to the latch
side of the door and centered 60 inches above the floor and leave the existing sign in
place on the door if removing it will damage the door.
Note: an additional sign may be mounted on the toilet room door but this cannot be
considered to be the accessible sign which must be mounted on the wall adjacent to
the latch side of the door.
Yes _____ No _____
Notes/Comments
42
ADA Emergency Shelter Checklist
H2. Does the door to the toilet room provide at least 32 inches clear passage
width when the door is open 90 degrees? [ADA Standards § 4.13.5]
H3. Is the hardware (e.g., lever, pull, panic bar) usable with one hand without
tight grasping, pinching, or twisting of the wrist?
[ADA Standards § 4.13.9]
If No, can the door be propped open without compromising privacy, or can the
hardware be modified by adding new accessible hardware, or adapting or replacing
hardware?
H4. On the pull side of the door, is there at least 18 inches clearance provided
on the latch side if the door is not automatic or power-operated?
[ADA Standards § 4.13.6, Fig. 25]
H5. If there is a raised threshold, is it no higher than 3/4 inch at the door and
beveled on both sides? [ADA Standards §§ 4.1.6(3)(d)(ii), 4.13.8]
If No, replace threshold with one with beveled sides or add a sloped insert.
H6. If the entry has a vestibule, is there a 30-inch by 48-inch clear floor space
inside the vestibule where a wheelchair or scooter user can be outside
the door swing? [ADA Standards § 4.13.7]
If No, possible solutions include leaving the inner door open or removing the outer
door.
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes __ No___ NA__
Yes _____ No _____
Notes/Comments
43
ADA Emergency Shelter Checklist
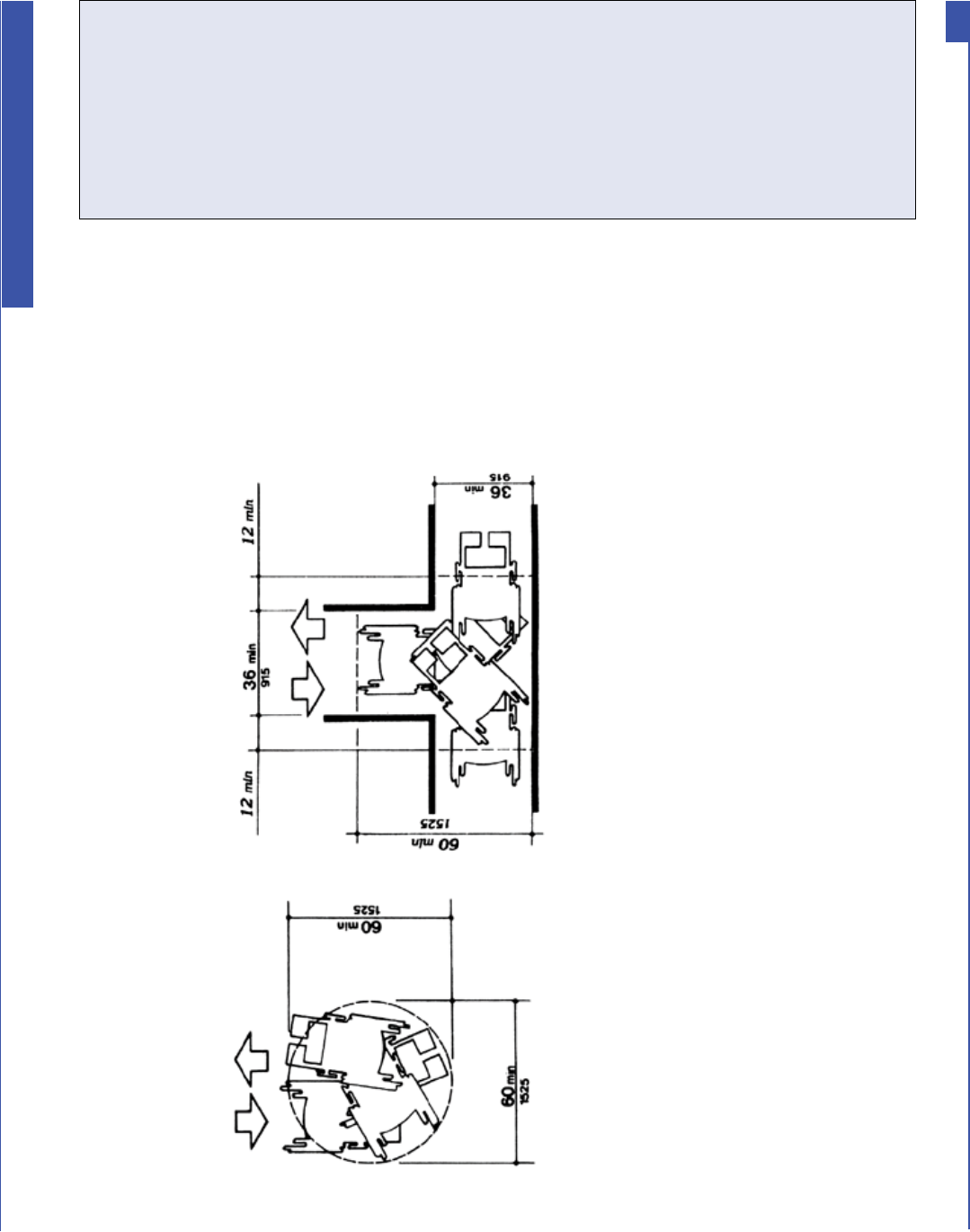
Minimum spaces for turning
H8. If lavatories are provided, does at least one have at least a 29 inch high
clearance under the front apron with the top of the rim no more than 34
inches above the floor? [ADA Standards § 4.19.2]
H9. Are the drain and hot water pipes for this lavatory insulated or otherwise
configured to protect against contact? [ADA Standards § 4.19.4]
Yes _____ No _____
H7. Inside the toilet room, is there an area where a person who uses a
wheelchair or other mobility device can turn around - either at least a
60-inch diameter circle or a “T”-shaped turn area as shown in the figures
below? [ADA Standards §§ 4.22.3; 4.2.3]
Yes _____ No _____
Notes/Comments
Yes _____ No _____
44
ADA Emergency Shelter Checklist
H10. Does this lavatory have controls that operate easily with one
hand, without tight grasping, pinching, or twisting of the wrist?
[ADA Standards § 4.19.5]
H11. If mirrors are provided, is the bottom of the reflecting surface for the
mirror at this lavatory no higher than 40 inches above the floor or is a full
length mirror provided? [ADA Standards § 4.19.6]
H12. For at least one of each type of dispenser, receptacle, or equipment, is
there clear floor space at least 30 inches wide x 48 inches long adjacent
to the control or dispenser (positioned either parallel to the control or
dispenser or in front of it)?
[ADA Standards §§ 4.23.7; 4.27.2; 4.2.5 and Fig 5; 4.2.6 and Fig 6]
H13. Is the operating control (switch, lever, button, or pull) of at least one of
each type of dispenser or built-in equipment no higher than 54 inches
above the floor (if there is clear floor space for a parallel approach)
or 48 inches (if there is clear floor space for a front approach)?
[ADA Standards §§ 4.23.7; 4.27.3; 4.2.5 and Fig 5; 4.2.6 and Fig 6]
H14. Are all built-in dispensers, receptacles, or equipment mounted so
the front does not extend more than 4 inches from the wall if the
bottom edge is between 27 inches and 80 inches above the floor?
[ADA Standards §§ 4.23.7; 4.27; 4.4.1; Fig. 8]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
45
ADA Emergency Shelter Checklist
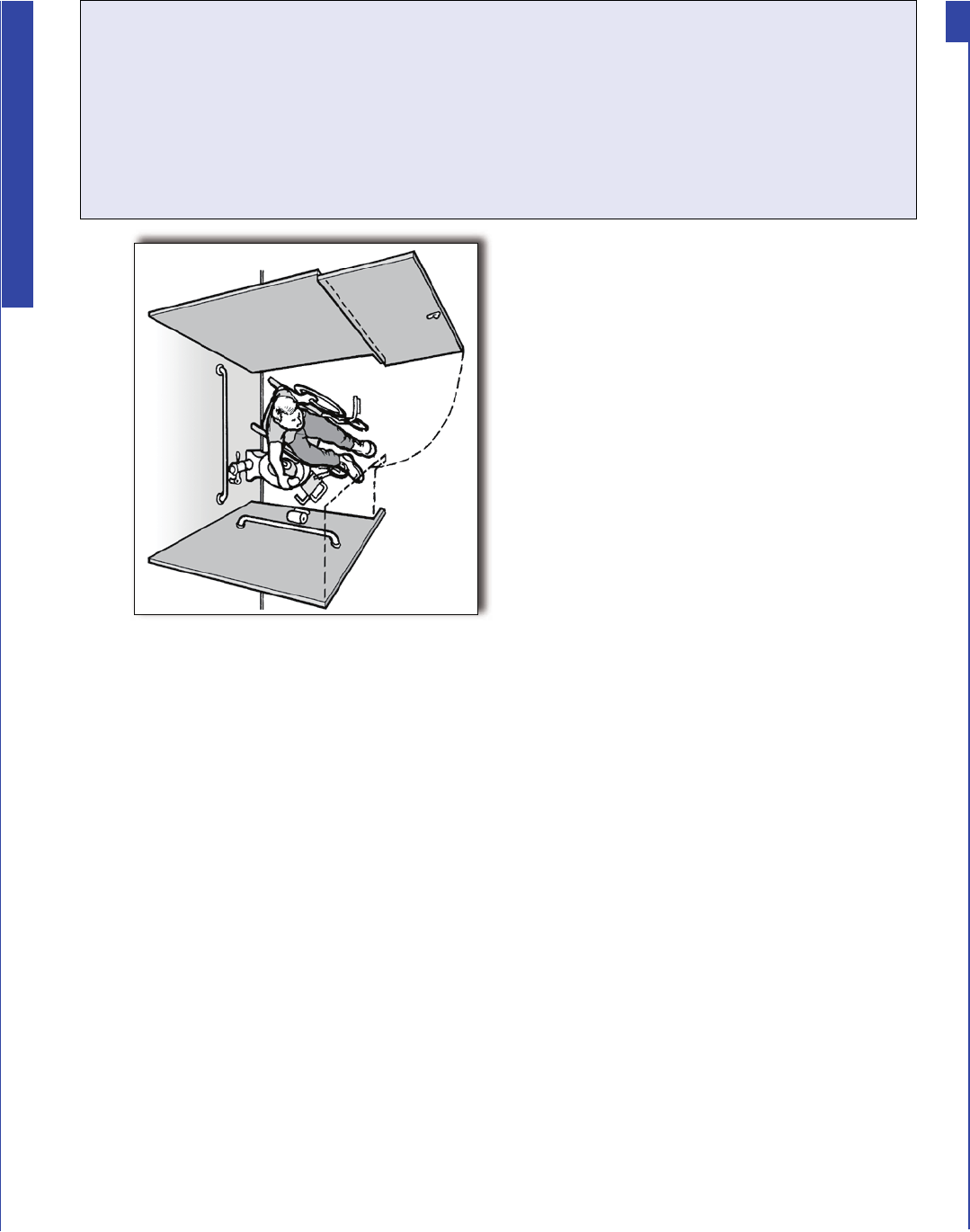
Toilet Stalls
H15. Is at least one wide toilet stall
provided with an outswinging
door, side and rear grab bars,
and clear space next to the
toilet?
[ADA Standards § 4.17]
If No, check to see if another toilet
room provides a wide accessible
toilet stall, note its location for
shelter planners, and answer all toilet
room questions with respect to that
toilet room.
Overhead view of an individual using a
wheelchair positioned beside a toilet in a
wide accessible stall.
Yes _____ No _____
H16. Is the toilet stall at least 60 inches wide and 56 inches deep
(wall mounted toilet) or 59 inches deep (floor mounted toilet)?
[ADA Standards § 4.17.3]
If No, note the width and depth of the stall. _________________
H17. Is at least 9 inches of toe clearance provided under the front wall and at
least one side wall of the toilet stall? [ADA Standards § 4.17.4]
H18. Is the centerline of the toilet 18 inches from the adjacent side wall?
[ADA Standards § 4.16.2; 4.17.3]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
46
ADA Emergency Shelter Checklist
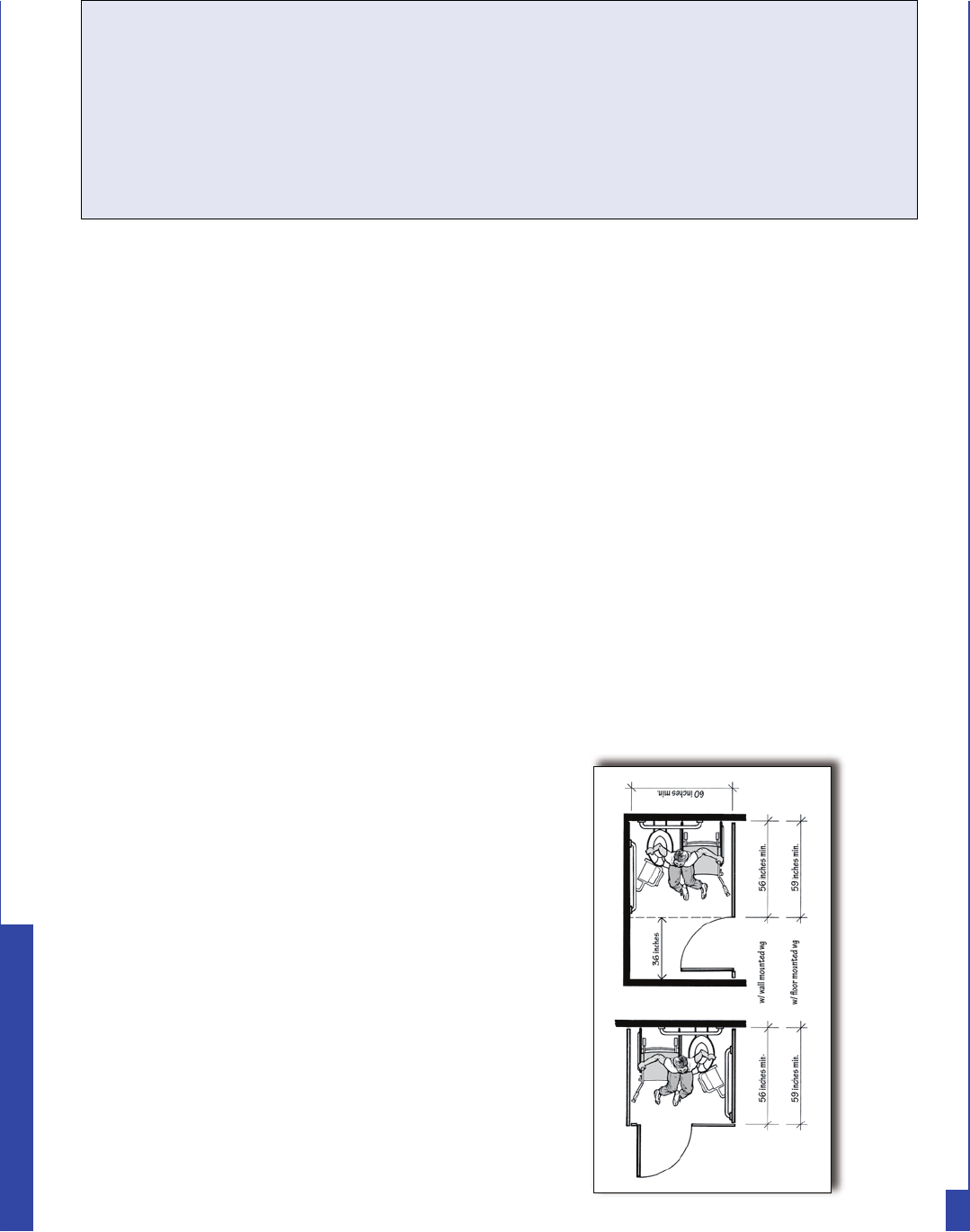
H19. Is the top of the toilet seat 17 inches to 19 inches above the floor?
[ADA Standards § 4.16.3]
H20. Is the flush valve located on the wide side adjacent to the lavatory or is
an automatic flush valve provided? [ADA Standards § 4.16.5]
H21. Is a horizontal grab bar at least 40 inches long securely mounted on
the adjacent side wall 33 to 36 inches above the floor with one end no
more than 12 inches from the back wall 33 to 36 inches above the floor?
[ADA Standards § 4.16.4; 4.17.6]
H22. Is a second horizontal grab bar at least 36 inches long securely mounted
on the back wall with one end no more than 6 inches from the side wall
33 to 36 inches above the floor? [ADA Standards § 4.16.4; 4.17.6]
H23. Is the door to the toilet stall located diagonally opposite, not directly in
front of, the toilet or on the opposite side wall from the wall with the
long grab bar? [ADA Standards § 4.17.3]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
Plan views showing minimum sizes of wide
accessible toilet stall
Yes _____ No _____H24. Unless the wide stall is
located at the end of a
row of toilet stalls,
does the door to this
wider stall open out?
[ADA Standards § 4.17.3]
47
ADA Emergency Shelter Checklist
H25. Is the clear width of the door at least 32 inches (measured between the
face of the door and the edge of the opening) when the door is open 90
degrees? [ADA Standards § 4.13.5]
H26. If there are 6 or more stalls in the restroom, is one of those stalls (in
addition to the wider stall noted above) exactly 36 inches wide with an
outswinging stall door that provides at least 32 inches of clear width?
[ADA Standards § 4.22.4]
H27. Does this 36-inch wide stall have horizontal grab bars on both of the side
partitions that are at least 36 inches long and 33 to 36 inches above the
floor? [ADA Standards § 4.22.4]
H28. Is the surface of the toilet seat in this 36-inch-wide stall 17 to 19 inches
above the floor? [ADA Standards §§ 4.16.3; 4.22.4]
H29. If a coat hook is provided is it mounted no higher than 54 inches above
the floor for a side approach or 48 inches above the floor for a front
approach? [ADA Standards § 4.25.3]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
48
ADA Emergency Shelter Checklist

7KH IROORZLQJ DUH ¿JXUHV LOOXVWUDWLQJ VRPH DFFHVVLEOH VKRZHU IHDWXUHV IURP WKH $'$ 6WDQGDUGV
Accessible Shower Stall
Minimum Size and Clearances
Accessible Shower Stall Grab Bars
and Seat, Shower, and Control Area
1RWH
)RU PDQ\ HPHUJHQF\ VKHOWHUV HYDFXHHV DUH QRW H[SHFWHG WR XVH VKRZHU RU EDWKLQJ IDFLOLWLHV GXH WR WKH VKRUW SHULRG WKH\ PD\ VWD\ DW WKH
VKHOWHU ,I SODQQLQJ IRU WKH VKHOWHU RSHUDWLRQ LQFOXGHV RIIHULQJ VKRZHU RU EDWKLQJ IDFLOLWLHV WKHQ WKRVH IDFLOLWLHV VKRXOG EH RQ DQ DFFHVVLEOH
URXWH DQG FKHFNHG IRU DFFHVVLELOLW\ )RU LQIRUPDWLRQ RQ WKH UHTXLUHPHQWV IRU DFFHVVLEOH VKRZHUV RU EDWKWXEV VHH WKH $'$ 6WDQGDUGV IRU
$FFHVVLEOH 'HVLJQ ZKLFK LV DYDLODEOH RQOLQH DW ZZZDGDJRY
49
ADA Emergency Shelter Checklist
I. Public Telephones
:KHQ SXEOLF WHOHSKRQHV DUH SURYLGHG WKHQ RQH RU PRUH DFFHVVLEOH SXEOLF WHOHSKRQHV VKRXOG EH SURYLGHG LQ DUHDV
VHUYLQJ VKHOWHU DFWLYLW\ DQG VHUYLFH DUHDV :KHQHYHU DFFHVVLEOH WHOHSKRQHV DUH SURYLGHG HDFK VKRXOG EH RQ DQ
DFFHVVLEOH URXWH ,Q VKHOWHUV LW LV FRPPRQ WR SURYLGH DGGLWLRQDO WHOHSKRQHV RQ WDEOHV RU GHVNV DQG VRPH RI WKHVH
WHOHSKRQHV VKRXOG EH DFFHVVLEOH
$ WH[W WHOHSKRQH DOVR FRPPRQO\ NQRZQ DV D 77< LV D GHYLFH WKDW DOORZV LQGLYLGXDOV ZKR DUH GHDI RU KDUG
RI KHDULQJ RU ZKR KDYH D VSHHFK GLVDELOLW\ WR FRPPXQLFDWH RYHU D WHOHSKRQH +DYLQJ DW OHDVW RQH 77< LQ DQ\
EXLOGLQJ WKDW KDV DW OHDVW IRXU SD\ SKRQHV SURYLGHV DFFHVV IRU SHRSOH ZKR DUH GHDI RU KDUG RI KHDULQJ
I1. If at least one public telephone or one bank of telephones is provided,
does at least one of each type of telephone (e.g., pay telephone,
intercom telephone, other telephone) have the following?
I1a. For a side approach (clear floor space at least 30 inches long x 48
inches wide), is the coin slot no higher than 54 inches above the
floor? [ADA Standards § 4.31.2, Fig. 44 (a)]
I1b. For a front approach (where clear floor space at least 30 inches
wide x 48 inches long), is the coin slot no higher than 48 inches
above the floor? [ADA Standards § 4.31.2, Fig. 44 (b)]
I2. Does the phone have volume controls? [ADA Standards § 4.31.5]
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
50
ADA Emergency Shelter Checklist
I3. If three or more telephones are located in one bank serving the shelter,
are a shelf and an electrical outlet provided at one telephone for use of a
portable TTY? [ADA Standards § 4.31.9 (2)]
I4. If four or more pay telephones are provided on the site, is there a TTY
(text telephone) provided at the shelter?
I5. Is there a sign at each pay phone or pay phone bank for the shelter
directing people to the nearest TTY? [ADA Standards § 4.30.7 (3);
4.31.9(3)]
Yes ____ No _____
If yes, location:
________________
Yes _____ No _____
Yes _____ No _____
Notes/Comments
A bank of two public telephones. The accessible
telephone is on the left and the telephone on the
right is equipped with a TTY.
51
ADA Emergency Shelter Checklist
J. Drinking Fountains
$SSUR[LPDWHO\ RI WKH GULQNLQJ IRXQWDLQV VHUYLQJ WKH VKHOWHU PXVW EH DFFHVVLEOH DQG ORFDWHG RQ DQ DFFHVVLEOH
URXWH $FFHVVLEOH GULQNLQJ IRXQWDLQV PXVW KDYH HQRXJK VSDFH IRU D SHUVRQ XVLQJ D ZKHHOFKDLU VFRRWHU RU RWKHU
PRELOLW\ GHYLFH WR XVH WKH GULQNLQJ IRXQWDLQ 7KH VSRXW DQG FRQWUROV RI WKH GULQNLQJ IRXQWDLQ PXVW EH QHDU WKH
IURQW HGJH 7KH FRQWUROV PXVW EH XVDEOH ZLWK RQH KDQG ZLWKRXW WLJKW JUDVSLQJ SLQFKLQJ RU WZLVWLQJ RI WKH ZULVW
7KH RWKHU RI GULQNLQJ IRXQWDLQV VHUYLQJ WKH VKHOWHU PXVW EH FRQÀJXUHG IRU XVH E\ SHRSOH ZKR KDYH GLIÀFXOW\
EHQGLQJ RU VWRRSLQJ ZKLOH VWDQGLQJ
:KHQ DQ REMHFW VXFK DV D GULQNLQJ IRXQWDLQ SURWUXGHV PRUH WKDQ IRXU LQFKHV LQWR WKH FLUFXODWLRQ SDWK WKH ERWWRP
HGJH PXVW EH DW LQFKHV DERYH WKH ÁRRU RU ORZHU VR WKH GULQNLQJ IRXQWDLQ LV QRW D KD]DUG WR SHRSOH ZKR DUH EOLQG
RU KDYH ORZ YLVLRQ
Notes/Comments
A person who uses a wheelchair is drinking from an
accessible drinking fountain. Beside the accessible
drinking fountain is a standard height fountain that
is usable by people who have difficulty bending or
stooping. The short wall beside the standard height
drinking fountain is cane detectable to guide people who
are blind or have low vision away from the standard
height fountain which, otherwise, would be a protruding
object hazard.
52
ADA Emergency Shelter Checklist
7KH IROORZLQJ TXHVWLRQV DSSO\ WR RI WKH GULQNLQJ IRXQWDLQV WKDW DUH SURYLGHG
J1. If the drinking fountain is a wall-mounted unit, is there clear floor space
at least 30 inches wide (36 inches if it is in an alcove) x 48 inches long
in front of the drinking fountain and at least 27 inches high under the
fountain so that a person using a wheelchair can get close to the spout
and controls? [ADA Standards § 4.15.5 (1), Figs. 4 (e) and 27 (b)]
J2. If the drinking fountain is a floor-mounted unit, is there clear floor space
at least 30 inches long x 48 inches wide (60 inches if it is in an alcove)
for a side approach to the drinking fountain so that a person using a
wheelchair can get close to the spout and controls even though the
fountain has no clear space under it?
[ADA Standards § 4.15.5 (2), Figs. 4 (e), 27 (c) and (d)]
J3. Is the top of the spout no higher than 36 inches above the floor and at
the front of the fountain or water cooler? [ADA Standards § 4.15.2]
J4. Does the water rise at least 4 inches high when no more than
5 pounds of force is applied to the controls of the fountain?
[ADA Standards §§ 4.15.3 and 4.15.4]
J5. Are the controls on or near the front of the unit and do they operate
with one hand without tight grasping, pinching, or twisting of the wrist?
[ADA Standards § 4.15.4]
J6. Is the bottom of the apron of the fountain 27 inches above the
floor so that it provides the space needed for a person who uses
a wheelchair to pull up under it but is not a hazard to people who
are blind or have low vision and use a cane to detect hazards?
[ADA Standards §§ 4.15.5 (1) and 4.4.1]
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
53
ADA Emergency Shelter Checklist
K. Eating Areas
$Q DFFHVVLEOH URXWH DW OHDVW LQFKHV ZLGH DQG ZLWKRXW VWHSV RU VWHHS VORSHV PXVW EH
SURYLGHG WR DQG WKURXJKRXW WKH IRRG VHUYLFH DQG HDWLQJ DUHDV RI WKH VKHOWHU 7KH DFFHVVLEOH
URXWH DOORZV SHRSOH ZKR XVH ZKHHOFKDLUV VFRRWHUV DQG RWKHU PRELOLW\ GHYLFHV WR JHW WR DOO
RI WKH IRRG DQG GULQN LWHPV LQ WKH VKHOWHU DQG WR DFFHVVLEOH WDEOHV DQG VHDWLQJ
A serving and eating area in a shelter are shown above. The shaded pathway
illustrates the accessible route connecting the entrance, serving areas,
accessible seats and tables, and the exit.
Notes/Comments
54
ADA Emergency Shelter Checklist
K1. Is there an accessible route, at least 36 inches wide, that connects each
of the shelter activity areas with the food service and eating areas (it
may narrow to 32 inches wide for up to 2 feet in length)?
[ADA Standards § 4.3.2(3)]
K2. Is there an accessible route that is at least 36 inches wide that connects
accessible tables with serving, condiment, and dispenser areas?
[ADA Standards § 5.3; 4.3.8]
K3. In each eating area, if tables with fixed seats are provided, do at least
5% of each type of table with fixed seats have accessible locations
with knee space at least 27 inches high, at least 19 inches deep, and at
least 30 inches wide with a table top 28 to 34 inches above the floor?
[ADA Standards § 5.1]
Note: If movable tables and chairs are used as shown, then locate at least 5% of the
tables adjacent to an accessible route. Tables can be relocated as needed during
operation of the shelter.
K4. If built-in food, drink, condiment, and tableware dispensers are provided,
are dispensers and operating controls mounted no higher than 54 inches
above the floor if clear floor space is provided for a side approach?
[ADA Standards § 5.5]
K5. If the operating controls are set back 10 to 24 inches from the front edge
of the counter or table are they no higher than 46 inches above the floor?
[ADA Standards § 5.5]
K6. If food service lines are provided, is an accessible route provided (at
least 36 inches wide) and are the tray slides no higher than 34 inches
above the floor? [ADA Standards § 5.5]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
55
ADA Emergency Shelter Checklist
L. Availability of Electrical Power
(PHUJHQF\ VKHOWHUV VKRXOG KDYH D ZD\ WR SURYLGH D EDFNXS SRZHU VXSSO\ ZKHQ WKH HOHFWULFDO VHUYLFH LV
LQWHUUXSWHG 7KH EDFNXS SRZHU LV QHHGHG WR SURYLGH UHIULJHUDWLRQ RI PHGLFLQHV RSHUDWLRQ RI VXSSOHPHQWDO
R[\JHQ DQG EUHDWKLQJ GHYLFHV DQG IRU FKDUJLQJ WKH EDWWHULHV RI SRZHU ZKHHOFKDLUV DQG VFRRWHUV ,QGLYLGXDOV
ZKRVH PHGLFDWLRQV FHUWDLQ W\SHV RI LQVXOLQ IRU H[DPSOH UHTXLUH FRQVWDQW UHIULJHUDWLRQ QHHG WR NQRZ LI D VKHOWHU
SURYLGHV VXSSOHPHQWDO SRZHU IRU UHIULJHUDWRUV RU LFHSDFNHG FRROHUV ,QGLYLGXDOV ZKR XVH PHGLFDO VXSSRUW
V\VWHPV VXFK DV VXSSOHPHQWDO R[\JHQ RU ZKR UHTXLUH SHULRGLF EUHDWKLQJ WUHDWPHQWV XVLQJ SRZHUHG GHYLFHV UHO\
RQ D VWDEOH VRXUFH RI HOHFWULFLW\ 7KHVH LQGLYLGXDOV
PXVW KDYH DFFHVV WR HOHFWULF SRZHU IURP D JHQHUDWRU
RU RWKHU VRXUFH RI HOHFWULFLW\ ZKLOH DW D VKHOWHU
,Q JHQHUDO LQ HDFK FRPPXQLW\ RU DUHD ZKHUH D
VKHOWHU LV SURYLGHG D IDFLOLW\ PXVW KDYH RQH RU PRUH
EDFNXS JHQHUDWRUV RU RWKHU VRXUFHV RI HOHFWULFLW\ VR
WKDW HYDFXHHV ZLWK D GLVDELOLW\ ZKR UHO\ RQ SRZHUHG
GHYLFHV FDQ KDYH DFFHVV WR HOHFWULFDO SRZHU ZKLOH DW
WKH VKHOWHU
Yes _____ No _____
Yes _____ No _____
OTHER ISSUES
Notes/Comments
L1. Is there a backup source of electrical power for the facility?
L2. Is there a refrigerator or other equipment, such as coolers with a good
supply of ice, at the shelter?
56
ADA Emergency Shelter Checklist
M. Single-User or “Family” Toilet Room
,Q PDQ\ VFKRROV DQG ODUJH IDFLOLWLHV ZKHUH HPHUJHQF\ VKHOWHUV DUH RIWHQ ORFDWHG VLQJOHXVHU WRLOHW URRPV PD\
EH SURYLGHG IRU VWDII ,Q WKRVH IDFLOLWLHV EXLOW RU DOWHUHG VLQFH WKH $'$ ZHQW LQWR HIIHFW VLQJOHXVHU WRLOHW URRPV
VKRXOG KDYH DFFHVVLEOH IHDWXUHV WKDW FRXOG EH XVHIXO GXULQJ VKHOWHU RSHUDWLRQ 7KHVH IHDWXUHV LQFOXGH DQ DFFHVVLEOH
HQWUDQFH DQG WXUQLQJ DQG PDQHXYHULQJ VSDFHV 7KHVH URRPV VKRXOG DOVR KDYH EHHQ EXLOW WR DOORZ JUDE EDUV
DFFHVVLEOH FRQWUROV DQG DFFHVVLEOH KDUGZDUH WR EH HDVLO\ LQVWDOOHG
$V SDUW RI WKH SODQQLQJ IRU RSHUDWLQJ DQ HPHUJHQF\ VKHOWHU IDFLOLWLHV RSHUDWRUV VKRXOG FRQVLGHU XVLQJ DQ DYDLODEOH
VWDII WRLOHW URRP LI SURYLGHG DV D VLQJOHXVHU RU ´IDPLO\µ WRLOHW URRP :KHQ SURYLGHG LQ DGGLWLRQ WR ODUJH
DFFHVVLEOH WRLOHW URRPV WKLV W\SH RI IDFLOLW\ SHUPLWV D SHUVRQ ZLWK D GLVDELOLW\ WR UHFHLYH DVVLVWDQFH IURP D SHUVRQ
RI WKH RSSRVLWH VH[
Notes/Comments
Yes _____ No _____
M1. If a sign is provided at the toilet room entrance (e.g. Men, Women, Boys,
Girls, etc.), is a sign with raised characters and Braille mounted on the
wall adjacent to the latch side of the door and centered 60 inches above
the floor? [ADA Standards § 4.1.3(16)(a)]
If No, install a sign with raised characters and Braille on the wall adjacent to the latch
side of the door and centered 60 inches above the floor and leave the existing sign in
place on the door if removing it will damage the door.
Note: an additional sign may be mounted on the toilet room door but this cannot be
considered to be the accessible sign which must be mounted on the wall adjacent to
the latch side of the door.
M2. Does the door to the toilet room provide at least 32 inches clear passage
width when the door is open 90 degrees? [ADA Standards § 4.13.5]
M3. Is the hardware (e.g., lever, pull, etc.) usable with one hand without tight
grasping, pinching, or twisting of the wrist? [ADA Standards § 4.13.9]
If No, add new accessible hardware or adapt/replace hardware.
Yes _____ No _____
Yes _____ No _____
57
ADA Emergency Shelter Checklist
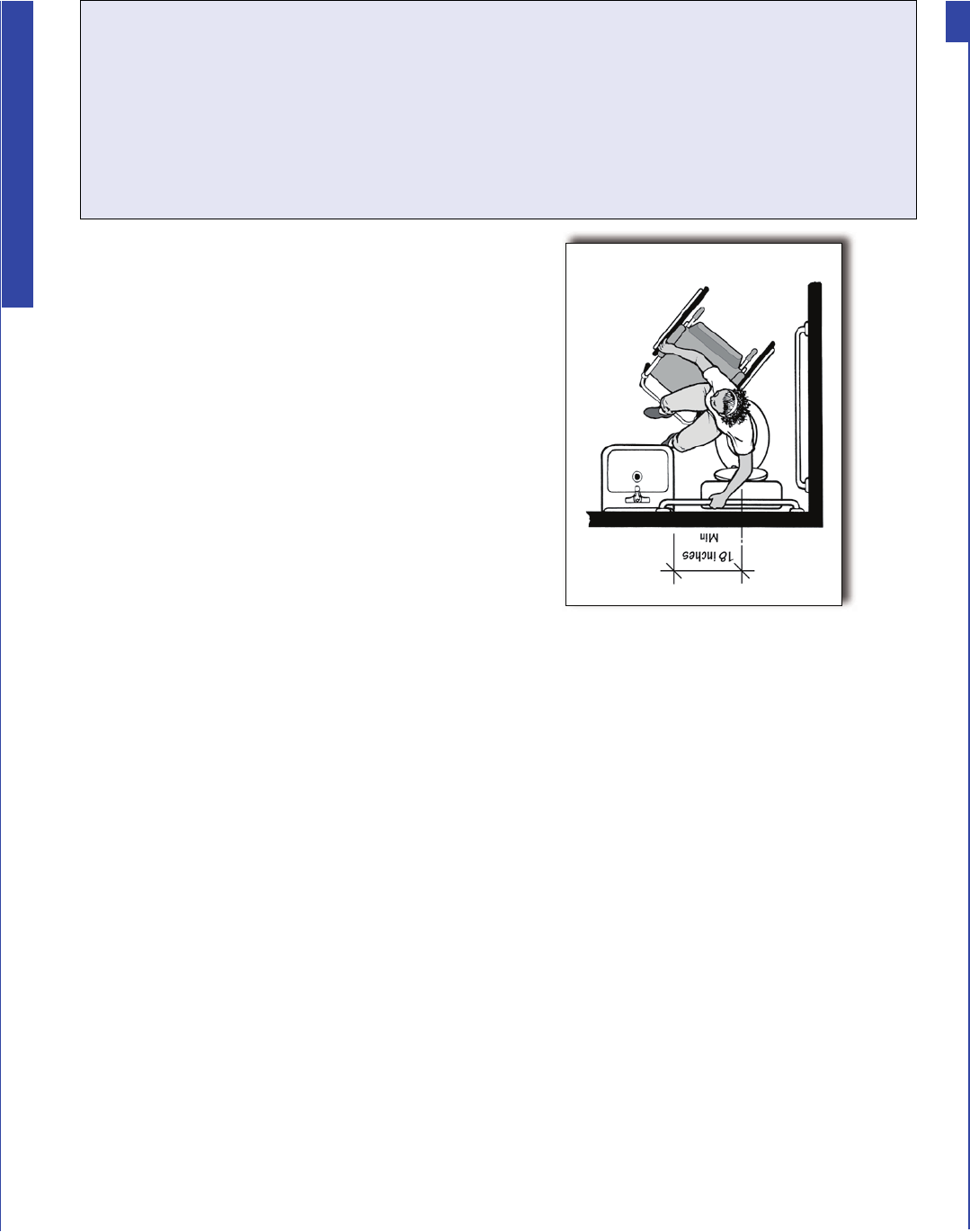
M4. On the latch, pull side of the door, is there at least 18 inches
clearance provided if the door is not automatic or power operated?
[ADA Standards § 4.13.6; Fig. 25]
M5. If there is a raised threshold, is it no higher than 3/4 inch at the door and
beveled on both sides? [ADA Standards §§ 4.1.6(3)(d)(ii); 4.13.8]
If No, replace threshold with one with beveled sides or add a sloped insert.
M6. Inside the room is there an area for a person who uses a wheelchair to
turn around - either a 60-inch diameter circle or a “T”-shaped turn area?
[ADA Standards §§ 4.22.3; 4.2.3]
M7. If the door swings into the room, does the door swing not
overlap the required clear floor space for the toilet or lavatory?
[ADA Standards §§ 4.22.2; 4.2.4.1]
Note: In the figure below the clear floor space for the toilet extends at least 66
inches from the back wall.
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
Yes _____ No _____
Plan view showing the minimum amount
of space required between the toilet and
the adjacent lavatory.
M8. Is there at least 18 inches
between the center of the toilet
and the side of the adjacent
lavatory?
[ADA Standards § 4.16.2; Fig.
28]
M9. Does the lavatory have at least
a 29-inch-high clearance under
the front edge and the top of
the rim no more than 34 inches
above the floor?
[ADA Standards § 4.19.2]
58
ADA Emergency Shelter Checklist
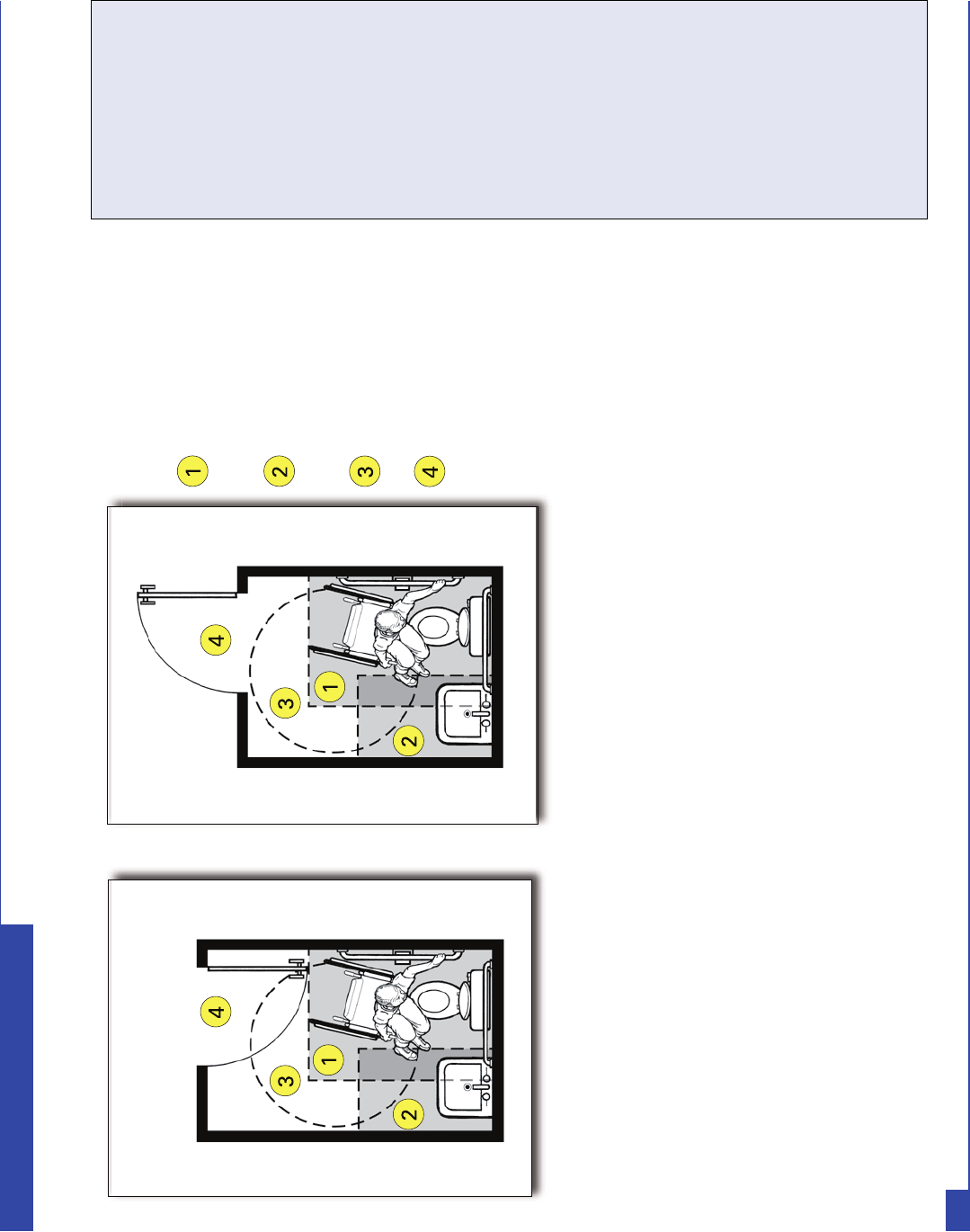
Notes:
48-inch minimum by
66-inch minimum clear
floor space for toilet
48-inch minimum by
30-inch minimum clear
floor space for lavatory
60-inch minimum
turning space
door swing
Yes _____ No _____
M10. Are the drain and hot water pipes for the lavatory insulated or otherwise
configured to protect against contact?
[ADA Standards § 4.19.4]
M11. Does that lavatory have controls that operate easily with one hand,
without tight grasping, pinching, or twisting of the wrist?
[ADA Standards § 4.19.5]
Plan view of a single-user toilet room showing the door swing not overlapping
the dark toned area indicating the clear floor space for the toilet and lavatory.
The door swing may overlap the turning space indicated by the circular area.
Notes/Comments
Yes _____ No _____
59
ADA Emergency Shelter Checklist
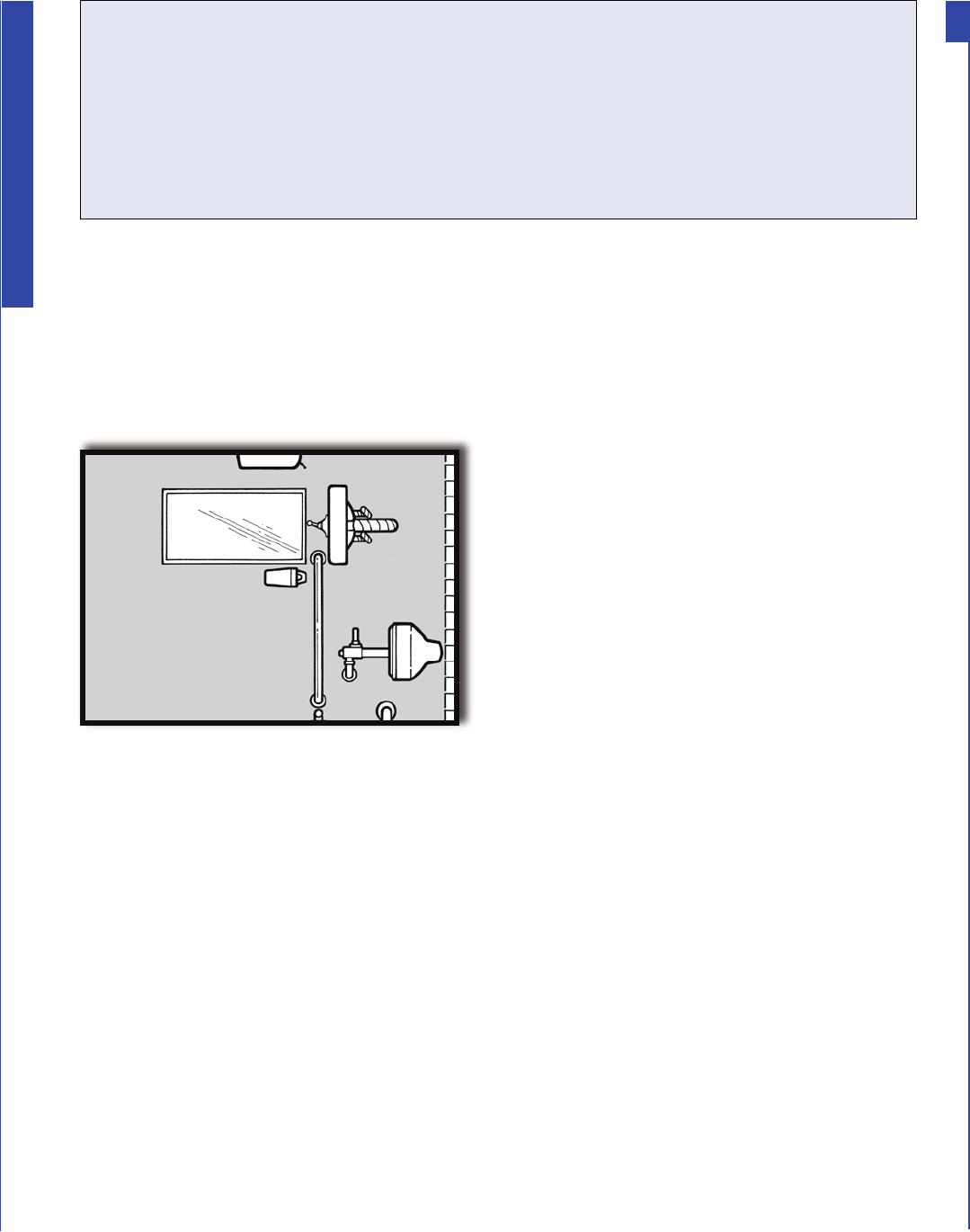
M12. If a mirror is provided, is the bottom of
the reflecting surface no higher than 40
inches above the floor or is a full length
mirror provided?
[ADA Standards § 4.19.6]
M13. For each type of dispenser, receptacle,
or equipment, is there clear floor space
at least 30 inches wide x 48 inches long
adjacent to the control or dispenser
(positioned either parallel to the control
or dispenser or in front of it)?
[ADA Standards §§ 4.23.7; 4.27.2; 4.2.5
and Fig 5; 4.2.6 and Fig 6]
M14. Is the operating control (switch, lever,
button, or pull) for each type of dispenser
or built-in equipment no higher than 54 inches above the floor (if there
is clear floor space for a parallel approach) or 48 inches (if there is clear
floor space for a front approach)?
[ADA Standards § 4.23.7; 4.27.3; 4.27.2; 4.2.5 and Fig 5; 4.2.6 and Fig 6]
M15. Are all built-in dispensers, receptacles, or equipment mounted so the
front does not extend more than 4 inches from the wall if the bottom
edge is between 27 inches and 80 inches above the floor?
[ADA Standards §§ 4.23.7; 4.27; 4.4.1; Fig. 8]
M16. Is the centerline of the toilet 18 inches from the adjacent side wall?
[ADA Standards § 4.16.2; 4.17.3]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
60
ADA Emergency Shelter Checklist
Front view of toilet, lavatory,
mirror and soap dispenser
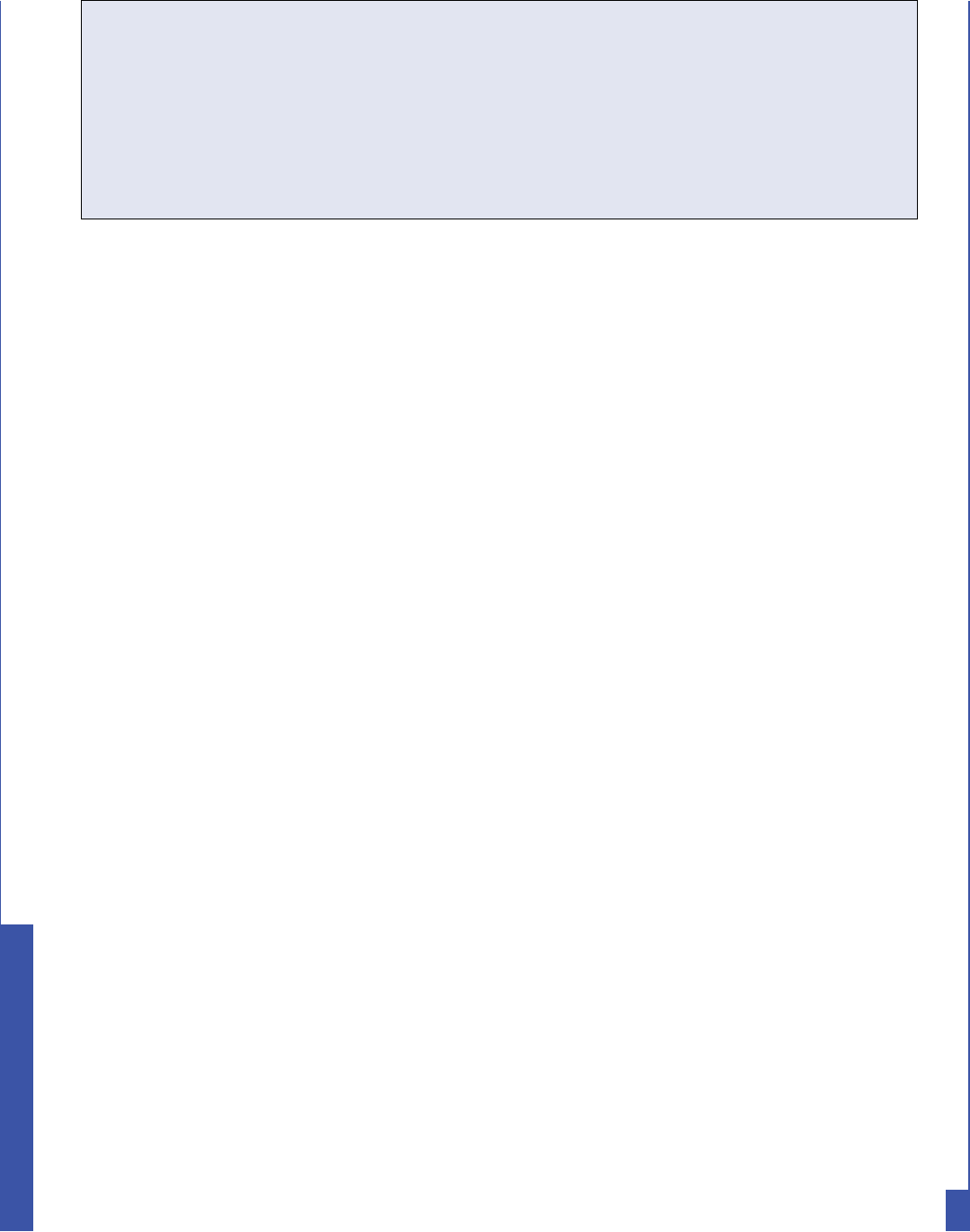
M17. Is the top of the toilet seat 17 to 19 inches above the floor?
[ADA Standards § 4.16.3]
M18. Is the flush valve located on the side adjacent to the lavatory?
[ADA Standards § 4.16.5]
M19. Is a horizontal grab bar at least 40 inches long securely mounted on
the adjacent side wall 33 to 36 inches above the floor with one end no
more than 12 inches from the back wall?
[ADA Standards §§ 4.16.4; 4.17.6]
M20. Is there a horizontal grab bar at least 36 inches long securely mounted
behind the toilet 33 to 36 inches above the floor with one end no more
than 6 inches from the side wall? [ADA Standards §§ 4.16.4; 4.17.6]
M21. If a coat hook is provided, is it mounted no higher than 54 inches
above the floor for a side approach or 48 inches above the floor for a
front approach? [ADA Standards § 4.25.3]
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Yes _____ No _____
Notes/Comments
Yes _____ No _____
61
ADA Emergency Shelter Checklist
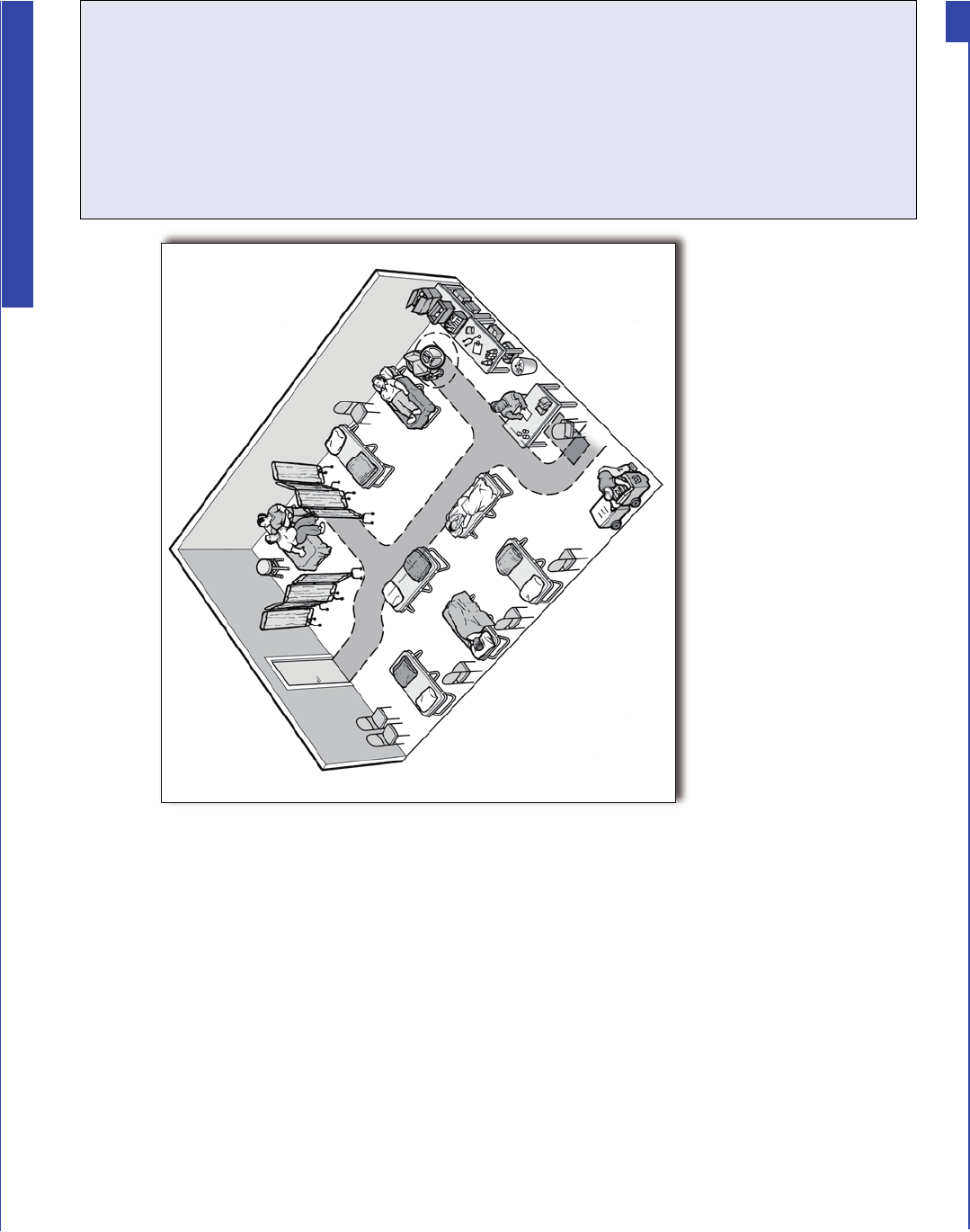
,Q PDQ\ VFKRROV ZKHUH HPHUJHQF\ VKHOWHUV
DUH RIWHQ ORFDWHG QXUVHV· URRPV RU RWKHU W\SHV
RI KHDOWK FDUH IDFLOLWLHV PD\ EH SURYLGHG
7KHVH KHDOWK FDUH IDFLOLWLHV VKRXOG EH RQ
DQ DFFHVVLEOH URXWH DQG KDYH DFFHVVLEOH
IHDWXUHV LQFOXGLQJ DQ DFFHVVLEOH HQWUDQFH
DQ DFFHVVLEOH URXWH WR WKH GLIIHUHQW W\SHV RI
VHUYLFHV RIIHUHG ZLWKLQ WKH PHGLFDO FDUH XQLW
WXUQLQJ DQG PDQHXYHULQJ VSDFHV DQG FRWV RU
EHGV WKDW DUH DW D KHLJKW WR ZKLFK SHRSOH ZKR
XVH PRELOLW\ GHYLFHV FDQ HDVLO\ WUDQVIHU
N. Health Units/Medical Care Areas
An overhead view of a medical care area with a shaded pathway
showing the accessible route shown and clear floor spaces.
N1. Is there an accessible route, at least 36 inches wide, that connects
each of the shelter activity areas with the health units and medical
care areas (it may narrow to 32 inches wide for up to 2 feet in length)?
[ADA Standards § 4.3.2(3)]
Yes _____ No _____
Notes/Comments
62
ADA Emergency Shelter Checklist
O. Accessible Portable Toilets
3RUWDEOH WRLOHWV DUH RIWHQ XVHG DW HPHUJHQF\ VKHOWHUV WR VXSSOHPHQW SHUPDQHQW
WRLOHW IDFLOLWLHV :KHQ SRUWDEOH WRLOHWV DUH SURYLGHG DW OHDVW RQH PXVW EH D XQLW
ZLWK DFFHVVLEOH IHDWXUHV WKDW LV ORFDWHG RQ DQ DFFHVVLEOH URXWH FRQQHFWLQJ LW ZLWK
WKH VKHOWHU )RU WKH HQWUDQFH WR DQ DFFHVVLEOH SRUWDEOH WRLOHW WR EH XVDEOH WKHUH
PXVW HLWKHU EH QR VWHS RU D UDPS PXVW EH LQVWDOOHG WKDW H[WHQGV H[WHQGV IURP WKH
KLQJH VLGH RI WKH GRRU WR DW OHDVW LQFKHV EH\RQG WKH ODWFK VLGH RI WKH GRRU
$FFHVVLEOH SRUWDEOH WRLOHWV VKRXOG VLPLODU IHDWXUHV WR D VWDQGDUG DFFHVVLEOH WRLOHW
VWDOO LQFOXGLQJ DQ DFFHVVLEOH GRRU VLGH DQG UHDU JUDE EDU FOHDU VSDFH QH[W WR WKH
WRLOHW DQG PDQHXYHULQJ VSDFH
A person using a wheelchair enters an accessible
portable toilet. The unit is positioned to provide a
flush entry from the accessible route.
63
ADA Emergency Shelter Checklist
115
Appendix 2
FORM: Contact Information for Shelter Services Providers
This is a small sample of the services you should have in place prior to an emergency or disaster
Services for Persons
Requiring FNSS Account Number Vendor Name Address Telephone
Communications Providers
Interpreters (Spanish, sign
language, etc.)
Television with Captioning
Information Technology/
Computer Services
TTY – TDD
Computer Assisted Real time
Translation (CART)
Note Taking
Medical Stafng Services
Onsite Nursing Services
Emergency Medical Services
Mental Health Services
Emergency Dental Services
Pharmaceutical Services
Resource Suppliers
O2
Dialysis
Constant Power Source
Blood Sugar Monitoring
116
Food Services
Special Diets
Caterer
Personal Assistance Services
Transportation Services
Para transit Services
Public Transportation
Service Animals
Emergency Veterinary
Services
Shelter Maintenance Services
Servicing for Accessible
Portable Toilets, Hand
Washing Units, etc.
Disposal of Bio-hazard
Materials
FNSS Equipment
Durable Medical Equipment
117
Appendix 3
Durable Medical Supply Sample List
DME (for children and adults)
Equipment Quantity Type
3 in 1 Commode for over toilet use (300 lb capacity) 5 Each
Assorted utensil holder 8 Each
Accessible Cots 100 Each
Beds, bariatric, on wheels, up to 600 lbs 6 Each
Bedside Commodes (3ea-w/300 lb capacity; 2ea-w/450 lb capacity) 5 Each
Canes, quad (6ea-small base; 2ea-large base; 2ea-bariatric) 5 Each
Canes, white 3 Each
Comfort box (1ea knit pant, 1ea t-shirt, 1ea pair socks, hygiene items) 10 Box
Crutches, adult 3 Pair
Crutches, pediatric 3 Pair
Dressing aid sticks 5 Each
Handheld Shower w/84” hose 4 Each
Independent Toilet Seats w/safety bars 4 Each
IV Pole 5 Castor 3 Each
Patient Lift w/2 mesh slings (450 lb cap) (Hoyer lift) 2 Each
Privacy Screen, 3 panel w/castors 10 Each
Refrigerator, counter height, no freezer (for meds) 2 Each
Sheets, at, tted for bariatric bed (200 thread count or higher) 6 Each
Shower Chair w/back rest (4ea-400 lb capacity; 2ea-Bariatric) 6 Each
Egg Crate Padding -10 beds and 6 wheelchairs 10/6 Each
Walker, dual release (4ea-standard w/wheels; 2ea-heavy duty w/wheels;
2ea-bariatric w/out wheels; 2ea-standard w/out wheels) 10 Each
Medical Cot w/mattress & half side rails 4 Each
Wheelchair ramps, portable (1ea-10’; 1ea -6’) 2 Each
Wheelchair transfer boards 8 Each
Wheelchairs, adult (7ea-w/footrests; 3ea-w/elevating leg rest) 4 Each
Wheelchairs, adult, extra large (to 450 lb capacity; 1ea-w/footrest;
1ea-w/elevating leg rest) 2 Each
Wheelchairs, pediatric (1ea-w/footrest; 1ea-w/leg rest) 2 Each
118
Appendix 4
Consumable Medical Supply Sample List
CMS (for children and adults)
Note 1: Planning estimate is based on 100 person shelter population for one week
Note 2: All liquid items must meet TSA standard (3.4 oz or less) in case of aerial evacuation
Item Description Quantity Notes
Antibacterial Wipes/
Towelettes
40 pack 100
Bag, plastic 13 gallon 100
Nutritional Supplemental
Drinks for Kids/Children
(over 12 months of age),
ready to drink (i.e.,Pedia-sure)
dispensed
by medical
authority in
shelter
28-120 . oz.
per day in no
larger than 8
oz bottles /
196 - 658 per
week
Magnifying Glasses
(standard)
2
Paper Cup Lids for 12 oz cups 1 case
Bendable Drinking Straws 1 case
Duct Tape 12 rolls
Waterproong Pads
(i.e. CHUX)
standard size 10 boxes of
24
Patient Care Gloves,
non-latex
disposable 6 boxes
Non-latex Cleaning Gloves disposable 4 boxes of
100
Bio-hazard Bags for medical
bio-waste
1 box of 24
Bleach, chlorine 2 gallons
Bucket, 2.5 gallon 10 each
Paper Towels 20 rolls
Hand Sanitizer 6 each large
Hand Sanitizer 100 each
individual
Baggies (large/small) 10 boxes each
Instant Ice pkg of 12 Self-contained, break to use
Instant Heat pkg of 12 Self-contained, break to use
119
Emesis Basin (shallow) each 12 Plastic 8.5”
Bedpans each 2 disposable
w/o cover
Resistant to stains and cracks. 350-pound
weight capacity. Contoured design molded
plastic for adults.
Bedpans each 10 disposable
w/o cover
Resistant to stains and cracks. Dimensions:
14” L x 11” W x 2.5”D. Weight capacity: 250
pounds.
Urinals - male each 8 disposable
w/cover
Plastic, disposable male urinal with cover -
translucent
Distilled Water (for
humidiers)
gallon 10
Nutrition drink for diabetics
(i.e. Glucerna)
each 48 (8 oz
bottles)
Plastic bottle contains ingredients that
contribute to blood glucose management and
support cardiovascular health. For people
with diabetes. For the use as a supplement,
snack, or meal as a part of a diabetes
management plan.
Nutrition Drink (i.e. Ensure) each 48 (8 oz.
reclosable
bottle)
Source of concentrated calories and is high
in protein to help patients gain or maintain
healthy weight. It is a complete and balanced
oral nutritional supplement that can be used
with or between meals or, in appropriate
amounts, as a meal replacement.
Trach Care Tray each 2 W-Forceps. Sterile, single-use. Compact and
disposable. All necessary components for
care and cleaning of trach site. Tray includes
removable basin, 2 latex-free gloves, trach
brush, drape, 36” twill tape, 2 cotton tipped
applicators, 2 pipe cleaners and 4 4”x4”
gauze and plastic forceps.
Scissors, blunt-end 2 each
Scissors, sharp and curved 2 each
Back Support each 2 Universal back support ts a range of sizes.
Wide, elastic support base. Overlapping
elastic compression panels. Adjustable and
removable shoulder straps.
Cervical Collar, universal size each 4 Soft foam collar is slightly contoured
for comfort. 1”-thick foam is covered
with stockinet and has loop/lock closure.
Universal style ts most. 2.5” wide at the
chin, ts neck circumference 12-22”.
Automatic Blood Pressure
Cuff, adult with batteries,
x-large
each 2 with x-large
adult cuff
Displays simultaneous readings of systolic
and diastolic blood pressure and pulse
Automatic Blood Pressure
Cuff, adult with batteries,
standard
each 2 with
standard cuff
Displays simultaneous readings of systolic
and diastolic blood pressure and pulse
120
Auto Blood Pressure Cuff,
child, with batteries
each 2 with child
cuff
Displays simultaneous readings of systolic
and diastolic blood pressure and pulse
Saline Solution (wound wash) each 12 A sterile saline solution (0.9%) for ushing
and cleansing supercial wounds
Pill Crusher 6 each
Pill Cutter 6 each
Diapers, adult x-large 3 cases of 20
Diapers, adult large 3 cases of 20
Diapers, adult medium 3 cases of 20
Diapers, adult small 3 cases of 20
Pull-Up Adult Diapers small 1 cases of 20
Saniwipe Disinfectant Towels 2 pkgs Textured cloth for a rigorous disinfection
in the most stringent medical environments
and continuous exposure to bodily uids and
blood
Sterile Gauze Sponges 4”x4” 2 boxes of
100
100 % cotton sponges of ne mesh gauze
for wound debriding, prepping, packing,
dressing, and general wound care
Sterile Gauze Sponges 2”x2” 2 boxes of 50 100 % cotton sponges of ne mesh gauze
for wound debriding, prepping, packing,
dressing, and general wound care
ABDs sterile wound
gauze pads
(not the blue
pads)
1 case
(approx 200)
ABD Pad Sterile 8”x10”. Soft, non-woven
layer for patient comfort and uff ller for
absorbency. All four edges are sealed to
prevent lint residue and leaking. Sterile, in
single peel back sleeve.
Ace Bandages (2”) rolls 2 boxes Economy Woven Elastic Bandage 2”x4.5yd.
Clip Closure 1ea/bx 1ea/cs ETO Latex-free
used for compression or securing of splints,
dressings, and ice packs. Economy and
standard REBs are standard grade woven
bandages that offer balanced stretch and
compression.
Ace Bandages (3”) rolls 2 boxes Economy Woven Elastic Bandage 3”x4.5yd.
Clip Closure 1ea/bx 1ea/cs ETO Latex Free
used for compression or securing of splints,
dressings, and ice packs. Economy and
standard REBs are standard grade woven
bandages that offer balanced stretch and
compression.
Ace Bandages (4”) rolls 2 boxes Economy Woven Elastic Bandage 4”x4.5yd.
Clip Closure 1ea/bx 1ea/cs ETO Latex Free
used for compression or securing of splints,
dressings, and ice packs. Economy and
standard REBs are standard grade woven
bandages that offer balanced stretch and
compression.
121
Ace Bandages (6”) rolls 2 boxes Economy Woven Elastic Bandage 6”x4.5yd.
Clip Closure 1ea/bx 1ea/cs ETO Latex Free
used for compression or securing of splints,
dressings, and ice packs. Economy and
standard REBs are standard grade woven
bandages that offer balanced stretch and
compression.
Application, cotton-tipped
(6” long, 100 per box)
2 boxes
Bandage Gauze Roll (2”) 6 dozen Cover-roll bandage 2”x10yd.
Bandage Gauze Roll (4”) 6 dozen Cover-roll bandage 4”x10yd.
Cotton Balls 4 bags of 50 100% cotton balls
Colostomy Appliance 2 packages Dependant on manufacturer
Colostomy Wafers 2 boxes of 10 Individually wrapped size 4”x4” wafer with
ange (skin protector)
Colostomy Paste 4 tubes (2 oz) IB Ostomy Paste 2 Oz Tube. Pectin based,
skin barrier paste helps protect the skin
around stomas and stulas to prevent skin
irritation and to ll-in uneven skin surfaces.
Colostomy Skin Preps 1 box of 50
wipes
No-Sting Skin-prep Wipes. Forms protective
lm to prepare skin for tapes and adhesives.
Colostomy Ileostomy Bags
(pouches)
11” drainable
colostomy/
ileostomy bag
(pouch)
1 boxes of 10 1 box of 10, cut to t, drainable colostomy/
ileostomy pouch
TELFA Dressings, sterile 2 boxes Absorbent cotton pad. Superior “Ouchless”
TELFA dressing won’t disrupt healing
tissue by sticking to wound. Each dressing
individually wrapped in peel-open envelope.
Ideal as primary dressing for lightly
draining wounds. Bonded on both sides with
perforated non-adherent lm; can be cut to
any shape without separating. Sterile. Size:
3”x4”.
General Antiseptic Cleansers
(i.e., BZK Towelettes)
2 boxes of
100
BZK Towelettes 5”x 7”. Used for general
antiseptic cleansing for patients and
staff, each towelette is saturated with
benzalkonium chloride 1:750. Contains no
alcohol. Latex-free.
Alcohol Prep Pads 4 boxes of
100
100 pads per box
K-Y Jelly 4 tubes large
Peroxide 4 bottles 16 oz
Betadine Scrub Solution 4 bottles 16 oz
Adhesive, non-allergic
(1” paper tape)
6 each 1” x 11yds.
122
Adhesive, non-allergic
(2” paper tape)
6 each 2” x 11yds.
Safety Pins 1 box Nickel-plated steel. Each pin closed. Secure
safety head. 1.75”. Box of 1440.
Medicine Cups 2 packages
100
1 oz
Hand Asepsis Towelettes 4 packages
pk/160
antimicrobial hand wipe
Batteries – assorted 1 package
each
AAA/AA/9 VOLT/C/D
Batteries - hearing aid 1 package
each
assorted
Spray Bottle plastic 4 each 6 oz
Blood Glucose Meter Kit 4 Allows for alternate site testing and stores up
to 300 test results. Includes meter, carrying
case, lancing device, 10 lancets, control
solution normal, alternate site testing cap.
Test Strips, diabetic 2 boxes of 50 50 strips per box
Velcro, double sided
(loop and hook)
1”,2” and 4” 6 rolls
(2 or each)
2 rolls ea of 1”, 2”, and 4”x 50yds.
Nebulizer 2 FIO (2) settings adjustable from 35% to
100%. It has ports for a feed set and an
immersion-type heater. Capacity: ~350ml^.
Isolation Mask 1 box of 50 Fluid-resistant, polypropylene outer facing
with ear loops
Foley Catheter 10 each Cath Foley Sil 12Fr 5cc. An All Silicone
Foley Catheter that is designed for enhanced
comfort and elimination of concerns
regarding potential health risks that may be
associated with repeated exposure to latex
devices.
Intermittent Catheter, male 25 each Cath Intmt Rdrbr 8Fr 16”. All-purpose,
urethral, X-ray opaque with funnel end
and round, hollow tip. Two opposing eyes.
Sterile. Size A: 16”^. Size B: 8Fr^.
Condom Catheters, male 25 each Cath Exterior Tex Ltx 2-Pc W-Fm. With
5.5”L x .75”W foam strap.
Intermittent Catheter, female 25each Intmt Pvc Pls Cath F 14 Fr 6.5”. Sterile.
Clear polyvinyl chloride with matte nish,
smooth rounded tip, funnel end. Size A:
~6.5”^. Size B: ~14 Fr^.
External Catheter, male 25 each Cath Ext Tex Ltx 2-Pc W-Fm. With 5.5”L x
.75”W foam strap.
123
Spray Adhesive, medical 5 cans Medical Adhesive Spray 3.2 oz. Increases
the adhesion to skin for pouches, wound
drainage collectors and fecal incontinence
systems.
Removal Wipes 1 box of 50 Universal adhesive remover for tapes,
adhesives, and hydrocolloid skin barriers.
Leg Bags, assorted sizes
small/medium/large
500ml x 3
600ml x 3
950ml x 3
9 (3 of each) T-Tap Leg Bag 500ml. Sterile. Secure,
comfortable, soft vinyl bags, with utter
valve and Velcro strap. Latex-free.
SizeA: ~500ml^. Style A:~With latex-free
tubing and connector^. Sterility: Sterile^.
Cannulas Nasal Oxygen
Tubes (disposable)
5 each Nasal cannula, extra soft, curved tip, with
7 ft. (213 cm.) crush - resistant tubing.
Regulators, 02 2 Oxygen Regulator with overall length less
than 4” and weighs just 6.9 oz. Lightweight
aluminum body with brass sleeve and brass
internals. Downward facing outlet port.
Bedside Drainage Collectors 3 2000cc drainage bag with drip chamber,
sample port and universal hanging device.
Power Strips 5 6 ft. length
Battery Chargers, universal 2 For recharging wheelchair batteries and other
battery-powered equipment.
Extension Cords 3 50 ft. length
T.E.D. Compression
Stockings
1 each
medium/
large/x-large
Support hose
Chemical-free Shampoo and
Body Wash
2 (8 oz
bottles)
Hypoallergenic cleanses - rinse free.
Contains Aloe Vera Gel, no alcohol.
Chemical-free Spray Cleaner 2 (8 oz
bottles)
Gentle cleanser contains Acemannan
Hydrogel - No rinse, Non-irritating
Air Pump (bicycle type) 1 For wheelchair tires w/composite head
tting. Presta, Schrader, and Woods/Dunlop
valves without switching internal parts.
124
125
Appendix 5
Guidance for Providing Personal Assistance Services
126

Guidance on Planning
for Personal Assistance
Services in General
Population Shelters
November 2010
128
129
Guidance on Planning for
Personal Assistance Services
in General Population
Shelters
Goal
Present guidance to State, local, and tribal governments regarding the need to provide Personal
Assistance Services (PAS) in general population shelters for children and adults with and without
disabilities who have access and functional needs.
Personal Assistance Services (PAS) are services that enable children and adults to maintain their usual
level of independence in a general population shelter.
Objectives
Present guidance on:
• Dening “ sufciency of services”
• Minimizing risk and exposure to litigation
• Identifying resources necessary to provide PAS to children and adults who require them
• Planning considerations for assisting children and adults requiring PAS
• Utilizing volunteers and leveraging existing systems that provide PAS
130

Page Section
133 1. Acronyms
133 2. Purpose
133 3. Disclaimer
134 4. Scope
134 5. Premise
135 6. Denition
137 7. Legal Foundation for PAS Guidance
140 7.1. Legal Authorities and References
141 8. PAS Guidance
142 8.1. Introduction
142 8.2. Sufciency of Care
142 8.3. Jurisdictional Variances
145 9.
Providing PAS during an Emergency or Disaster
145 9.1. Leveraging Services
145 9.1.1. Identifying Existing Community Resources
147 9.1.2. Recruiting, Orienting, and Training PAS Providers
148 9.1.3. Providing PAS Resources and Supplies
151 10. Glossary
152 11. Operational Tools
Contents
Guidance on Planning for Personal
Assistance Services in General
Population Shelters
132
133
Guidance on Planning for
Personal Assistance Services
in General Population Shelters
1. Acronyms
AED Automated External Debrillator
ADA Americans with Disabilities Act
CIL Center for Independent Living
CART Computer Assisted Real time Translations
CBO Community-Based Organization
CMS Consumable Medical Supplies
DME Durable Medical Equipment
EOC Emergency Operations Center
FEMA Federal Emergency Management Agency
FNSS Functional Needs Support Services
PAS Personal Assistance Services
TDD Telecommunications Device for the Deaf
TTY Teletypewriter
VOAD Voluntary Organizations Active in Disasters
2. Purpose:
The purpose of this document is to provide guidance to emergency managers and shelter planners
for the development of Personal Assistance Services (PAS) for children and adults with and without
disabilities who have access and functional needs and require PAS to maintain their usual level of
independence in a general population shelter. These guidelines, based on Federal law directives,
identify methods of achieving a lawful and equitable program.
3. Disclaimer:
This document provides guidance to assist emergency managers and shelter planners in understanding
the requirements related to providing PAS to children and adults who require them in general
population shelters. It is not intended to establish new legal obligations, alter existing obligations, or
constitute a legal interpretation of the statutes that are the basis of the guidance materials.
Listing of an agency’s or organization’s processes/procedures as an operational tool in this guidance
does not constitute a recommendation or endorsement of the resource. In addition, information
presented in an operational tool may have been summarized, modied, and/or combined with other
cited sources.
This PAS Guidance is an appendix of the Guidance on Planning for Integration of Functional
Needs Support Services in General Population Shelters and should be used in conjunction with that
document.
134
4. Scope:
This document is intended to provide guidance regarding the PAS necessary to meet Federal
requirements of integrating children and adults with and without disabilities who have access and
functional needs into every aspect of emergency planning and response. It is intended to be used in
conjunction with general population shelter standard operating procedures to ensure that all shelter
residents benet equally from programs, services, and activities. It provides a context for providing
PAS in light of other existing plans and describes a process to use in any planning effort. These
guidelines are scalable and can be applied to urban, suburban, and rural localities with multiple or
limited resources.
The PAS guidance recognizes that many jurisdictions across the country operate general population
shelters and many have already developed emergency operations plans; however, the PAS Guidance
is designed to help both novice and experienced emergency managers and shelter planners ensure
inclusion of people with disabilities and/or access and functional needs.
Children and adults with and without disabilities who have access and functional needs and require
PAS have the same right to services in general population shelters as other residents. Emergency
managers and shelter planners have the responsibility to plan for shelter services and facilities that are
accessible.
5. Premise:
Every day, Americans provide extraordinary levels of assistance to individuals of all ages and
situations. Formal and informal PAS are provided in virtually every community to enable children
and adults with and without disabilities who have access and functional needs to maintain their
independence and fully participate in all aspects of home and community life.
Historically, gaps have existed in planning for and meeting the need for PAS in general population
shelters. This has resulted in disparate treatment and the denial of full and equal services. This
guidance is provided to ensure that children and adults with disabilities and/or access and functional
needs are no longer turned away from general population shelters and inappropriately placed
in special needs or medical shelters. Addressing these gaps benets the entire community and
maximizes resources.
135
6. Denition:
Personal Assistance Services (PAS) are formal and informal services provided by paid personnel,
personal attendants, friends, family members, and volunteers that enable children and adults to
maintain their usual level of independence in a general population shelter. These services (when
necessary) may include, but are not limited to, assisting with:
• Basic personal care:
◦ Grooming
◦ Eating
◦ Bathing
◦ Toileting
◦ Dressing and undressing
◦ Walking
◦ Transferring
◦ Maintaining health and safety
• Activities of daily living:
◦ Taking medications
◦ Shopping for groceries
◦ Communicating
◦ Accessing programs and services
The Operational Tools in this document are excerpts and examples taken from agency and
jurisdictional documents throughout the United States. While they are not meant to dictate a State’s
policies or procedures, they do present ideas and practices that can be adapted to t each State’s
specic needs.
Operational Tool #1 Personal Assistance Services
Denition
of PAS
Personal Assistance Services – Also known as personal attendant services, attendant
care services, and personal care services (PCS) – These services include “people or
devices that assist a person with a physical, sensory, mental, or learning disability with
tasks that the person would perform for himself or herself if he or she did not have a
disability.” It includes a range of assistance provided to persons with disabilities and
chronic conditions, which enables them to accomplish tasks that they would normally
do for themselves if they did not have a disability.
PAS are provided to people of all ages to help with Activities of Daily Living (ADLs),
such as grooming, eating, bathing, dressing and undressing, toileting, or Instrumental
Activities of Daily Living (IADLs), such as taking medications, shopping for
groceries, communicating, and accessing programs and services.
PAS are generally classied into two categories:
• Informal (unpaid) services provided by family members, friends, and
neighbors
• Formal services that are paid either directly out-of-pocket, or by public payers,
private insurance, or other sources
Source
Center for Personal Assistance Services, University of California, San Francisco, Cal.;
http://www.pascenter.org
136
137
7. Legal Foundation
For PAS Guidance
The Stafford Act and Post-Katrina Emergency Management Reform Act (PKEMRA), along with
Federal civil rights laws, mandate integration and equal opportunity for people with disabilities in
general population shelters.
To comply with Federal law, those involved in emergency management and shelter planning should
understand the concepts of accessibility and nondiscrimination and how they apply in emergencies.
Following are key nondiscrimination concepts applicable under Federal laws, and examples of how
these concepts apply to all phases of emergency management.
1. Self-Determination – People with disabilities are the most knowledgeable about their own
needs.
2. No “One-Size-Fits-All” – People with disabilities do not all require the same assistance and do
not all have the same needs.
• Different types of disabilities affect people in different ways. Preparations should be made
for individuals with a variety of functional needs, including individuals who use mobility
aids, require medication or portable medical equipment, use service animals, need
information in alternate formats, or rely on a personal attendants.
3. Equal Opportunity – People with disabilities must have the same opportunities to benet from
emergency programs, services, and activities as people without disabilities.
• Emergency recovery services and programs should be designed to provide equivalent
choices for people with disabilities as they do for individuals without disabilities. This
includes choices relating to short-term housing or other short-term and long-term disaster
support services.
4. Inclusion – People with disabilities have the right to participate in and receive the benets of
emergency programs, services, and activities provided by governments, private businesses,
and nonprot organizations.
• Inclusion of people with various types of disabilities in planning, training, and evaluation
of programs and services will ensure that all people are given appropriate consideration
during emergencies.
5. Integration – Emergency programs, services, and activities typically must be provided in an
integrated setting.
• The provision of services such as sheltering, information intake for disaster services, and
short-term housing in integrated settings keeps individuals connected to their support
system and personal attendants and avoids the need for disparate service facilities.
6. Physical Access – Emergency programs, services, and activities must be provided at locations
that all people can access, including people with disabilities.
• People with disabilities should be able to enter and use emergency facilities, and access the
provided programs, services, and activities. Facilities typically required to be accessible
include: parking, drop-off areas, entrances and exits, security screening areas, toilet rooms,
bathing facilities, sleeping areas, dining facilities, areas where medical care or human
services are provided, and paths of travel to and from and between these areas.
138
7. Equal Access – People with disabilities must be able to access and benet from emergency
programs, services, and activities equal to the general population.
• Equal access applies to emergency preparedness, notication of emergencies, evacuation,
transportation, communication, shelter, distribution of supplies, food, rst aid, medical
care, housing, and application for and distribution of benets.
8. Effective Communication – People with disabilities must be given information that is
comparable in content and detail to that given to the general public, as well as accessible,
understandable, and timely.
• Auxiliary aids and services may be needed to ensure effective communication. These
may include pen and paper or sign language interpreters through on-site or video and
interpreting for individuals who are deaf, deaf-blind, hard of hearing, or have speech
disabilities. Individuals who are blind, deaf-blind, have low vision, or have learning
disabilities may need large print information or assistance with reading and lling out
forms.
9. Program Modications – People with disabilities must have equal access to emergency
programs and services, which may entail modications to rules, policies, practices, and
procedures.
• Service staff may need to change the way questions are asked, provide reader assistance to
complete forms, or provide assistance in a more accessible location.
10. No Charge – People with disabilities may not be charged to cover the costs of measures
necessary to ensure equal access and nondiscriminatory treatment.
• Examples of accommodations provided without charge to the individual may include:
ramps; cots modied to address disability-related needs; a visual alarm; grab bars;
additional storage space for mobility aids and other equipment; lowered counters or
shelves; Braille and raised letter signage; a sign language interpreter; a message board;
assistance in completing forms and providing documents in Braille; large print or audio
recording.
See FEMA’s Non-discrimination Principles of the Law:
http://www.fema.gov/oer/reference/principles.shtm
The Americans with Disabilities Act of 1990 (ADA), the Rehabilitation Act of 1973 (RA), and the
Fair Housing Act (FHA), their regulations and agency guidance, as well as State counterparts, among
others, dene the scope of FNSS. These hallmarks of equal opportunity for people with disabilities
include:
• The implementation and execution of a general policy of nondiscrimination on the basis of
disability
• Sheltering persons with disabilities in the most integrated setting appropriate to the needs of
the individual, which is the same setting people without disabilities enjoy in almost every case
• Reasonable modications of policies, practices, and procedures to ensure nondiscrimination,
with reasonableness judged in light of nondiscrimination principles applied in emergent
circumstances
• The provision of auxiliary aids and services to ensure effective communication, with primary
consideration of the aid or service given to the individual with a disability
• Elimination of eligibility criteria, discriminatory administrative methods, paternalistic safety
requirements, and surcharges where discrimination results
• The selection of accessible sites for the location of general population emergency shelters,
the construction of architecturally-compliant mass care shelters and elements, and required
physical modications to ensure program accessibility in existing facilities

139
The U.S. Department of Justice has provided guidance to State and local governments advising that
people with disabilities should be housed in mass care shelters even if they are not accompanied
by their personal care aides. “Some people with disabilities use personal care assistance for
activities of daily living, such as eating, dressing, routine health care, and personal hygiene needs.
One question that frequently arises is whether people with disabilities who use attendant care can be
appropriately housed in mass care shelters. In most instances, they can. Most people with disabilities
who use attendant care are not medically fragile and do not require the heightened level of medical
care provided in a special needs or medical shelter.
In the past, some shelter operators maintained policies that prevented people with disabilities who
regularly use attendant care from entering mass care shelters unless they were accompanied by their
own personal care attendants. These policies denied access to many people with disabilities.
During emergencies, many personal care attendants – like other people – evacuate or shelter with
their own families instead of staying with their clients. Shelter operators should provide support
services in mass care shelters to accommodate people with disabilities who are not medically
fragile but need some assistance with daily living activities unless doing so would impose an undue
nancial and administrative burden. Such assistance can be provided by medical personnel or trained
volunteers.”
1
1
http://www.ada.gov/pcatoolkit/chap7shelterprog.htm
140
7.1. Legal Authorities and References
ADA Best Practices Tool Kit for State and Local Governments, Chapter 7, Emergency Management
under Title II of the ADA (2007), Addenda 1-3, and the Introduction to Appendices 1 and 2 (Attached
as Exhibit 1); Titles II, III, and V of the Americans with Disabilities Act of 1990, 42 U.S.C. §§ 12101-
12103, 12131-12134, 12181-12188, and 12201-12213, as amended by the ADA Amendments Act
of 2008.
Nondiscrimination on the Basis of Disability in State and Local Government Services,
28 C.F.R. pt. 35.
Nondiscrimination on the Basis of Disability by Public Accommodations and in
Commercial Facilities, 28 C.F.R. pt. 36.
The Americans with Disabilities Act Title II Technical
Assistance Manual (1993) and Supplement (1994).
The Americans with Disabilities Act Title III
Technical Assistance Manual (1993) and Supplement (1994).
Section 504 of the Rehabilitation Act of 1973, 29 U.S.C. §§ 794, as amended.
Enforcement of
Nondiscrimination on the Basis of Handicap in Programs or Activities Conducted by the Federal
Emergency Management Agency, 44 C.F.R. pt. 16.
Enforcement of Nondiscrimination on the Basis
of Handicap in Programs or Activities Conducted by the Department of Justice, 28 C.F.R. pt. 39.
Nondiscrimination on the Basis of Handicap in Programs or Activities Receiving Federal Financial
Assistance, 45 C.F.R. pt. 84 (Department of Health and Human Services).
Nondiscrimination on
the Basis of Handicap in Programs or Activities Receiving Federal Financial Assistance, 34 C.F.R.
pt. 104 (Department of Education).
Nondiscrimination Based on Handicap in Federally Assisted
Programs and Activities of the Department of Housing and Urban Development, 24 C.F.R. pt. 8.
Title VIII of the Civil Rights Act of 1968 (“Fair Housing Act”), as amended, 42 U.S.C. §§ 3601-3631.
Discriminatory Conduct Under the Fair Housing Act, 24 C.F.R. pt. 100.
The Architectural Barriers Act of 1968, as amended, 42 U.S.C. §§ 4151-4157.
Construction and
Alteration of Public Buildings, 41 C.F.R. pt. 101-19.
The Homeland Security Act of 2002, 6 U.S.C. §§ 101-557, as amended.
The Robert T. Stafford Disaster Relief and Emergency Assistance Act, 42 U.S.C. §§ 5121-5206, as
amended.
Federal Disaster Assistance, 44 C.F.R. pt. 206.
The Post-Katrina Emergency Management Reform Act, 6 U.S.C. § 761(d), as amended
Emergency managers and shelter planners are encouraged to investigate their applicable State laws
for additional requirements.
141
8. PAS Guidance
This document outlines common scenarios that general population shelter managers and operators
may encounter during emergencies and disasters, and presents guidance to emergency managers
and shelter planners on providing Personal Assistance Services (PAS) so people who require these
services may benet from the sheltering program. In most instances, PAS have not been provided in
general population shelters up to this point. Clarication of legal obligations, recognition of the need
to plan for all members of the community, and favorable outcomes resulting from implementation of
best practices have all supported the benets of planning for the delivery of PAS in general population
shelters. The guidance provided in this document suggests strategies to assist in planning for PAS.
PAS is provided in virtually every community on a daily basis. Consequently, resources to plan for
shelter-based PAS are readily available locally.
The Operational Tools in this document are excerpts and examples taken from agency and
jurisdictional documents throughout the United States. While they are not meant to dictate a State’s
policies or procedures, they do present ideas that can be adapted to t each State’s specic needs.
Throughout this document “State” is used to refer to a U.S. State or U.S. territory.
142
8.1. Introduction
Historically, PAS for children and adults with disabilities have not been provided in general
population shelters. During disasters, children and adults with and without disabilities who have
access and functional needs have been re-directed to “special needs” or medical shelters. In some
instances, the only shelters that would admit people with disabilities have been remotely located and
have caused children and adults who required PAS to be separated from their families, friends, or
personal attendants.
To help address the lack of PAS in general population shelters, this guidance has been developed to
assist emergency managers and shelter planners in establishing plans to address the provision of PAS
to children and adults who require these services in order to maintain their independence.
Emergency managers and shelter planners need to include information in their State’s emergency
response plan related to identifying, developing, and providing PAS in general population shelters.
8.2. Sufciency of Care
General population shelters should be prepared to provide sufciency of care for all residents. These
services include PAS. As with other shelter services, it is imperative that plans to provide PAS are in
place prior to an emergency or disaster.
Because PAS are offered in virtually every community, emergency managers and shelter planners can
begin planning for these services at the local level by involving people who routinely use and provide
these services. (Reference Leveraging Services below). In many instances, the individuals and/
or agencies that are experienced PAS providers will be willing and able to continue providing those
services in a shelter setting. However, should these services be unavailable, the State should plan to
use volunteers and/or paid providers to ensure a sufciency of care when PAS is needed.
8.3. Jurisdictional Variances
State codes and standards must, at a minimum, meet Federal requirements, but can be more
comprehensive. The ADA and other Federal laws, including the Stafford Act, the Rehabilitation
Act, the Fair Housing Act, and the Architectural Barriers Act, provide afrmative obligations
and prohibitions of discrimination on the basis of disability. No State or local government, or its
contractors, in providing services may, by law, policy or contract, provide services below those
standards without violating Federal law. This does not mean that a State or local government cannot
enact laws and ordinances or provide services, obligations, and prohibitions that extend beyond these
standards to ensure even greater access. A common example would be to provide twice as many as
the required number of accessible parking spaces and access aisles.
143
Because each jurisdiction (State, local, and tribal) is different and the laws, rules, and regulations that
apply to each State and community vary, there is no single national plan for providing PAS in general
population shelters. Emergency managers and shelter planners should use existing information
regarding the local laws, rules, regulations, and demographics of their State and/or community to
develop a plan to provide PAS. At a minimum, the plan should consider and address:
• Existing information regarding the day-to-day utilization of PAS
• Service provider-to-shelter resident ratios based on projected need for PAS and availability of
State and local resources to provide these services in a shelter setting
• The development of plans and agreements to utilize resources (e.g., DME and CMS) currently
available to provide required PAS
• Potential gaps in current information regarding the need for PAS, including:
◦ Transient populations such as migrant workers and tourists
◦ Individuals who receive informal PAS from family and friends
◦ Plans for providing PAS in regional evacuation areas where local PAS resources may be
insufcient, destroyed, or damaged
Emergency managers and shelter planners need to include in their State plan, options for providing
PAS outside the area where an emergency or disaster occurs in the event that it is not possible to
shelter residents in their home community.
Operational Tool #2 Demographic Information – by State
Sample of available information
regarding the number of persons
who have a disability or have
difculty performing self-care
activities in California
1,109,000 persons (3.9%) of Californians have difculty with
self-care activities and/or other routine activities
Source Center for Personal Assistance Services, University of
California, San Francisco, Cal; http://www.pascenter.org
Note: Click on Need for PAS; click on Disability Statistics
Operational Tool #3 Demographic Information – by county
Sample of available
information regarding the
number of persons who have
a disability or have difculty
performing self-care activities
in Travis County, Texas
1.3% of the population ages 16 through 64 have a “self-care
disability” and 2.2% have a “go outside disability.” 12% of the
population, ages 65 and above, have a “self-care disability” and
18.9% have a “go outside” disability.” These percentages in either
category should not be added together since people with a “self-
care disability” are often a subset of the “go outside disability.”
Source Center for Personal Assistance Services, University of California,
San Francisco, Cal.; http://www.pascenter.org
Note: Click on Need for PAS; click on Disability Statistics;
click on Disability Statistics; click on Disability Prevalence for
Counties; click on Texas; click on Travis County
144
145
9. Providing PAS During an
Emergency or Disaster
9.1. Leveraging Services
9.1.1. Identifying Existing Community Resources
Long before an emergency or disaster occurs, emergency managers and shelter planners should begin
working closely with individuals in the community who require PAS. Emergency managers and
shelter planners should also reach out to organizations and providers that routinely provide PAS to
children and adults with disabilities. It is essential that appropriate PAS are available when needed in
an emergency situation. Suggested Community-based Organizations (CBO) providing or advising on
PAS on a regular basis include, but are not limited to:
• Center for Independent Living (CIL)
• Home health organizations
• Rehabilitation centers
• Home and community living organizations
• Respite providers
• Mental health organizations
• Developmental disability organizations
• Aging organizations
• Advocacy groups
• Protection and advocacy agencies
• The Salvation Army
• Faith-based organizations
• Colleges and universities
• Vocational service agencies
• Rehabilitation agencies
• American Red Cross
• Personnel from nursing homes and assisted living facilities
• Personnel from hospitals and health care systems
146
Operational Tool #4 Identifying PAS Resources
Locating PAS Assistance and advice on providing PAS is available from:
• The National Council on Independent Living
• Association of Programs for Rural Independent Living
• Independent Living Research Utilization
Source http://www.ncil.org
1710 Rhode Island Avenue Northwest/Fifth Floor
Washington, D.C. 20036
Source http://www.april-rural.org
Source http://ilru.org/
Operational Tool #5 Identifying Community-based PAS
Involvement and
cooperation with local
community-based
organizations (CBOs)
• Identify and build relations with the CBOs already linked to local
government through service contracts
• Meet to discuss potential areas for CBOs involvement in care and
shelter operations
• Encourage CBOs to cooperatively use their resources (e.g., food,
transportation, health/mental health services) to ensure that care and
shelter services meet the PAS needs within the community
• Determine the support that CBOs will need to keep services going
during a disaster or emergency
• Focus additional meetings around specic planning issues
• Involve CBOs in disaster planning, training, and exercises sponsored
by State and local governments
• Support CBOs by:
◦ Giving them priority status for supplies or resources
◦ Having a CBO representative in the EOC
◦ Establishing a memorandum of understanding with selected CBOs
◦ Developing agreements with CBOs stipulating that the CBOs will
make staff experienced in providing PAS as required during an
emergency or disaster
Source A Guide for Local Jurisdictions In Care and Shelter Planning, Alameda
County Operational Area Emergency Management Organization,
September 2003
http://www.cdsscounties.ca.gov/coplanners/res/pdf/doc16.pdf

147
9.1.2. Recruiting, Orienting, and Training PAS Providers
Emergency managers and shelter planners should include in their plans strategies to recruit, enroll,
orient, and communicate with PAS providers.
Recruitment strategies can include:
• Utilizing existing PAS providers
• Publicizing the need for PAS providers in malls, universities, service club newsletters, State
and local websites, and public services announcements
• Targeting individuals with interests and/or skills to provide PAS
• Implementing a simple process for volunteering
Enrollment strategies can include:
• Obtaining basic identifying information on providers
• Completing criminal background checks, when necessary
Orientation strategies can include:
• Dening PAS
• Stating what tasks PAS providers will be expected to perform
• Providing comprehensive information about how to:
◦ Set-up exercises for PAS providers to practice the tasks they will be expected to perform
◦ Develop a training curriculum that includes how to provide assistance in:
▪ Basic personal care
Grooming
Eating
Bathing
Toileting
Dressing and undressing
Walking
Transferring
Medications, DME, and CMS
Maintaining health and safety
▪ Effective communication
▪ Accessing programs and services
Operational Tool #6 PAS Workers and Personal Attendants
PAS Workforce Project Presents information regarding PAS workers and personal attendants,
including who they are, what they provide, and tools and support
necessary to carry out their tasks
Source Center for Personal Assistance Services; http://pascenter.org
Note: Click on Workers and Caregivers
Implementing these or similar strategies will increase the likelihood that PAS providers will be
available when they are needed and that they will be assigned appropriate PAS responsibilities during
an emergency or disaster.
148
Operational Tool #7 Non-professionals Providing PAS
Red Cross Family
Caregiving
Includes information for non-professionals who are providing PAS including:
• Home safety
• Caregiving Skills
• Body Mechanics
• Personal Care
• Healthy Eating
• Caring for the Caregiver
• Legal and Financial
• Dementia
• Caregiving Resources
Source Be Red Cross Ready, American National Red Cross, Safety Series Vol.1,
2007; www.mississippi-redcross.org
Operational Tool #8 PAS Training
Providing information,
training, and experience
to persons providing PAS
Prior to an emergency, plan how staff will be instructed in their roles
and responsibilities during a disaster. Include in the training:
• A denition of “emergency”
• When an emergency plan will be implemented
• Roles and responsibilities of essential and non-essential PAS
providers
• Procedures for educating clients about the preparedness plan
• Information for PAS providers regarding how they can work
with the local shelter management during an emergency
Source Virginia Department of Health, Ofce of Licensure and Certication,
Emergency Preparedness Planning for Hospice and Home Care
Providers, Effective September 1, 2006
http://www.vdh.state.va.us/OLC/Laws/documents/HCO%20and%20
HSP%20emergency%20prep.pdf
9.1.3. Providing PAS Resources and Supplies
In addition to identifying staff and volunteers to provide PAS, emergency managers and shelter
planners should include in emergency plans, several options for pre-identifying resources and supplies
that will be critical to assisting children and adults who require PAS. This includes DME, CMS, and
the services that support the provision of PAS. At a minimum, plans should address:
• Processes for locating, purchasing, and storing as much of the DME and CMS as possible and
practical to meet the needs of children and adults who require PAS
• Agreements with providers to ensure that necessary DME and CMS will be available during
an emergency or disaster
• Agreements with communities to ensure that if one community is severely damaged or
destroyed, necessary DME and CMS will be available
• Identifying and leveraging resources of assistive technology exchanges, lending, and
reutilization programs

149
Operational Tool #9 Durable Medical Equipment (DME) List
DME (for children
and adults)
See the “Guidance on Planning for Integration of Functional Needs Support
Services in General Population Shelters” for the Federally-approved DME
list.
Source FEMA: Guidance on Planning for Integration of Functional Needs Support
Services in General Population Shelters; Appendix 3: Durable Medical
Supply Sample List
Operational Tool #10 Consumable Medical Supplies (CMS) List
CMS (for children
and adults)
See the “Guidance on Planning for Integration of Functional Needs Support
Services in General Population Shelters” for the Federally-approved CMS
list.
Source FEMA: Guidance on Planning for Integration of Functional Needs Support
Services in General Population Shelter; Appendix 4: Consumable Medical
Supply Sample List
Operational Tool #11 Communication Devices
Communication
Devices – not
inclusive
• Sound amplication aids: TTY/TDD Phones
• Computer/laptop with capability for video relay communication
• Cap Tel Phones (for captioning)
• Computer Assisted Real-time Translation
• Hearing aid batteries of different sizes (including batteries for cochlear
implants)
Source Guidance on Planning and Responding to the Needs of People with Access
and Functional Needs, California Emergency Management Agency, Ofce for
Access and Functional Needs; http://www.calema.ca.gov/
Note: Click on Ofce for Access and Functional Needs
Source BCFS: www.bcfs.net/fnssrecommendations
Operational Tool #12 Resource for Assistive Technology
Reuse of assistive
technology
There is at least one Federally funded program in every State that engages
in the reuse of assistive technology. These programs are also connected to
other entities in the State that reuse assistive technology so they can serve as
a central point of contact for emergency managers and shelter planners.
Source http://www.resnaprojects.org/nattap/at/statecontacts.html
(contact information only)
Source http://www.resnaprojects.org/nattap/at/statecontacts.html#al
(contact information)
In addition to DME, CMS, and communication devices, emergency managers and shelter planners
should ensure that the services necessary to support the provision of PAS are identied and
consistently available.
150
Operational Tool #13 Legal Authority for PAS
Legal Authority
for PAS
Federal agencies may, on the direction of the president, provide assistance
essential to meeting immediate threats to life and property resulting from a major
disaster, including:
• Medicine, durable medical equipment, goods, and other consumables
• Emergency medical care; emergency mass care shelter; and provision of
food, water, medicine, and durable medical equipment
In any emergency, the president may assist State and local governments in the
distribution of medicine, food, and other consumable supplies and emergency
assistance.
Federal authority for provision of PAS can be found in the reference below.
Source Source Sections 403 (a)(2) and (3)(B) and 502(a)(7) of the Robert T. Stafford
Disaster Relief and Emergency Assistance Act, 42 U.S.C. §§ 5121-5206, as
amended. Federal Disaster Assistance, 44 C.F.R. pt. 206.
http://www.fema.gov/about/stafact.shtm
During an emergency or disaster, some shelters may have no source of emergency power generation,
while others may have only a limited source. Emergency managers and shelter planners should take
whatever steps are necessary to plan for providing an alternate source of power in the event of an
outage.
Many children and adults who require PAS depend on battery-powered assistive devices for mobility,
including wheelchairs and scooters. The batteries in these mobility aids must frequently be recharged
or they stop functioning. Without these mobility aids, children and adults with disabilities lose their
ability to move independently. This may render them unable to participate in some services offered by
the shelter and more dependent on assistance from others.
In addition, plans should include arrangements with multiple providers for an ongoing supply of
oxygen and access to dialysis facilities. Not having these services available will result in a failure to
provide residents sufcient care and may result in an unnecessary surge on medical facilities. Many
people live independently and require very little assistance when they are able to access oxygen,
dialysis, and other life sustaining aids and services.
Emergency managers and shelter planners should make arrangements for these services well before
an emergency or disaster, and should include back-up plans in the event that primary providers cannot
follow through as promised. DME and CMS may be available from a State, regional, FEMA, and/or
HHS stockpile.
When a shelter does not have in place the provisions for necessary DME, CMS, and communication
devices and services, operating a general population shelter that includes children and adults requiring
PAS becomes much more difcult and seriously threatens the well being of shelter residents.
Every community will have residents and visitors needing PAS in a disaster. Planning to meet these
needs in advance strengthens the ability of the community to meet the needs of its members and
maximize limited resources.
151
10. Glossary
Cap Tel
A communication system that provides written captions of everything a caller says on a built-in
display.
CART
Computer Assisted Real-time Translation
Consumable Medical Supplies (CMS)
Medical supplies (medications, diapers, bandages, etc.) that are ingested, injected, or applied and/
or are one time use only
Durable Medical Equipment (DME)
Medical equipment (e.g., walkers, canes, wheelchairs) used by persons with a disability to
maintain their usual level of independence
Sufciency of care
The services that shelter residents, including children and adults with disabilities and/or access or
functional needs, require in order to maintain a pre-disaster level of health and independence
TDD
Telecommunications Device for the Deaf
TTY
Teletypewriter
Universal/Accessible Cot
A Universal/Accessible cot that meets the following recommended criteria:
• Height 17”-19” without [below] the mattress(es)
• Width – minimum 27”
• Weight capacity – 350+ pounds
• Flexible head and feet position
• Rails, if any, must be positioned or moveable in such a way as to allow for wheelchair
access. No IV pole.
152
11. Operational Tools*
Operational Tool #1 Personal Assistance Services
Operational Tool #2 Demographic Information – by State
Operational Tool #3 Demographic Information – by county
Operational Tool #4 Identifying PAS Resources
Operational Tool #5 Identifying Community-based PAS
Operational Tool #6 PAS Workers and Personal Attendants
Operational Tool #7 Non-professionals Providing PAS
Operational Tool #8 PAS Training
Operational Tool #9 Durable Medical Equipment (DME) List
Operational Tool #10 Consumable Medical Supplies (CMS) List
Operational Tool #11 Communication Devices
Operational Tool #12 Resource for Assistive Technology
Operational Tool #13 Legal Authority for PAS
* Operational Tools – The Operation Tools in this document are excerpts and examples taken from
agency and jurisdictional documents throughout the United States. While they are not meant to
dictate a State’s policies or procedures, they do present ideas and practices that can be adapted to t
each State’s specic needs.
153
154
155
Appendix 6
One Day Menu for General Population Shelters Providing
Functional Needs Support Services
ONE DAY MENU
One day
menu
Regular Diabetic Reduced Sodium Pureed Infant
Breakfast Orange Juice 6 oz
Grits
Scrambled Egg
Bacon
Biscuit/Margarine
Coffee or Tea
Milk skim or 2% 8oz
Orange juice 6 oz
Grits
Scrambled Egg
Bacon
Biscuit/Margarine
Coffee or Tea
Milk skim 8oz
Orange Juice 6 oz
Grits
Scrambled Egg – no
salt when cooking
Biscuit/Margarine
Coffee or Tea
Milk skim 8oz
Orange juice 6 oz
Grits
Scrambled Egg
pureed
Biscuit/Margarine
pureed
Coffee or Tea
Milk skim 8oz
Formula
and baby
food
Lunch Hamburger on bun
Potato chips
Peaches in juice
Cookie
Ketchup/Mustard
Coffee or Tea
Milk skim or 2% 8 oz
Hamburger on bun
Potato chips
Peaches in Juice
Sugar free cookie
Ketchup/Mustard
Coffee or Tea
Milk skim 8 oz
Hamburger (no salt
when cooking) on
bun
Potato chips
Peaches in juice
Cookie
Ketchup
Coffee or Tea
Milk skim 8 oz
Hamburger on bun
pureed
Mashed potatoes
Peaches in juice
pureed
Cookie pureed
Ketchup/Mustard
Coffee or Tea
Milk skim 8 oz
Formula
and baby
food
Dinner Turkey and Gravy
Dressing
Carrots
Pears in juice
Bread 2 slices
Margarine
Coffee or Tea
Milk skim or 2% 8 oz
Turkey and Gravy
Dressing
Carrots
Pears in juice
Bread 2 slices
Margarine
Coffee or Tea
Milk skim 8 oz
Turkey and low
sodium gravy
Dressing
Carrots
Pears in juice
Bread 2 slices
Margarine
Coffee or Tea
Milk skim 8 oz
Turkey and gravy
pureed
Dressing pureed
Carrots pureed
Pears in juice pureed
Bread 2 slices
Margarine
Coffee or Tea
Milk skim 8 oz
Formula
and baby
food
Source BCFS; www.bcfs.net/fnssrecommendations
156
Appendix 7
FORM: Resident Health Care Information
RESIDENT’S HEALTH CARE RECORD
Name of Resident:
Assigned Resident #: DOB: Sex:
Date Time Complaint Treatment
© 2010 BCFS
158
Appendix 8
FORM: Medication Administration Record
MEDICATION ADMINISTRATION RECORD
Name of Guest:
Shelter: DOB:
Allergies:
Date Time Medication Dosage Route
Nurse’s
Initials
Printed Nurse’s Name: Initials
Printed Nurse’s Name: Initials
Printed Nurse’s Name: Initials
© 2010 BCFS
160
Appendix 9
FORM: Transportation Request Information
TRANSPORTATION REQUEST FORM
Date request: Time:
Name of Requester:
Name of Resident needing transportation:
Assigned Resident #:
Additional Family Members to be Transported:
Address of Pick Up Location:
Purpose of the Trip: Medical Need Return Home Other
Name of Destination:
Contact at the Discharge Destination:
Contact Phone Number:
Any special equipment or transportation (wheelchair van, stretcher, etc.) needed for persons listed above:
Luggage to be transported if at discharge:
Date and Time for pick up:
Date and Time for return to shelter if applicable:
Transportation arranged: Yes No
If no, explain:
Requester Notied of Action on Request: Yes No
Date and Time of Notication:
Notied by Whom:
© 2010 BCFS
162
Appendix 10
FORM: Resident Discharge Information
DISCHARGE FORM
Staff Information
Shelter Name:
Date:
Name of Person Filling out Form:
Personal Information
Last Name: First Name:
Resident ID: Address:
Phone No:
Caregiver Name (if applicable):
Relationship: Phone No:
Number of Individuals discharged with guest:
List Individuals discharged with guest:
Name Resident ID Relationship
Destination
□ Home □ Nursing facility □ Hospital □ Hotel
□ Apartment □ Friend □ Family □ Caregiver
□ Shelter □ Retirement Facility □ Hospice
Other:
Name of Destination Facility:
Address: Phone No:
Email: Fax No:
Alternate Point of Contact: (Name & Phone #):
PLEASE CONTINUE FILLING OUT THE FORM ON THE BACK
© 2010 BCFS
Transportation Needs
□ Car □ Bus □ Accessible Vehicle □ Ambulance
Other:
Discharge Checklist
□ Electricity to area
□ Guest is physically able to make the trip
□ Roads clear to destination
Equipment and Supplies Returned with Guest:
□ Medication □ Equipment □ Personal Items
Medication/ Equipment:
Forwarding Address of Resident:
Additional Comments:
GUEST SIGNATURE:
DATE: TIME:
© 2010 BCFS
