Department of Health and Human Services
Office of the Assistant Secretary for Planning and Evaluation
http://aspe.hhs.gov
ASPE
ISSUE BRIEF
THE AFFORDABLE CARE ACT:
PROMOTING BETTER HEALTH FOR WOMEN
June 14, 2016
By Adelle Simmons, Jessamy Taylor, Kenneth Finegold, Robin Yabroff, Emily Gee, and Andre Chappel
ASPE thanks the Agency for Healthcare Research and Quality, particularly Claudia Steiner, for their
contributions to this report.
The Affordable Care Act promotes better health for women through the law’s core tenets of access,
affordability, and quality. For example, the law’s provisions have expanded coverage through the
Health Insurance Marketplaces and Medicaid expansions; made coverage more affordable through
premium tax credits and by eliminating gender differences in premiums in the individual and small-
group insurance markets; and improved quality of coverage by eliminating lifetime and annual dollar
limits on Essential Health Benefits and requiring coverage of recommended preventive services and
maternity care. Continued implementation of the Affordable Care Act will play a significant role in
promoting the health and well-being of women across the lifespan. This report is organized into three
sections that describe how health care access, affordability, and quality of care have improved for
women since enactment of the Affordable Care Act.

ASPE Issue Brief Page 2
ASPE Office of Health Policy
Key Highlights:
Health insurance coverage increased: Between 2010 and 2015, the uninsured rate among women
ages 18 to 64 decreased from 19.3 percent to 10.8 percent, a relative reduction of 44 percent.
Coverage gains through the Marketplaces: About 12.7 million Americans selected affordable,
quality health plans through the Health Insurance Marketplaces for 2016 coverage. Of that total
number, 6.8 million (53.6 percent) are women and girls.
Preventive services at no out-of-pocket cost: Because of the Affordable Care Act, an estimated
55.6 million women with private insurance are guaranteed coverage of recommended preventive
services with no out-of-pocket costs.
Improved access to care: The percentage of women with a usual source of care has increased since
2010, particularly among young women (a 5.2 percentage point increase between 2010 and 2014),
Black women (a 5.1 percentage point increase), Hispanic women (a 6.5 percentage point increase),
and women with incomes at or below 400 percent of the federal poverty level (a 3.8 percentage point
increase).
Reductions in delayed care: From 2010 to 2014, the proportion of young women who reported
delaying or forgoing care because of cost concerns dropped by 3.4 percentage points; the proportion
dropped by 3.5 percentage points among Black women, 4.1 percentage points among Hispanic
women, and 3.0 percentage points among women with incomes at or below 400 percent of the
federal poverty level.
Protection from hospitalization costs: Women in Medicaid expansion states were much less likely
to be uninsured during a hospitalization than women in non-expansion states. The total number of
inpatient hospital discharges accounted for by uninsured women ages 19-64 declined by 50.5 percent
between 2010 and 2014 in Medicaid expansion states versus 4.0 percent in non-expansion states.
Improved outcomes for pregnant women and newborns: Babies born full-term have better
outcomes than babies who are electively delivered in the early term period. Between 2010 and 2013,
there was a 70.4 percent reduction in early elective deliveries among hospitals participating in the
HHS Strong Start for Mothers and Newborns Initiative. As of May 2014, more than 25,000 early
elective deliveries were prevented.
Better drug coverage under Medicare: More than 6 million women with Medicare prescription
drug coverage have saved $11 billion on prescription drugs since 2010.
ASPE Issue Brief Page 3
ASPE Office of Health Policy
I. Improving Access to Health Insurance Coverage
In October 2013, at the start of the first (2014) open enrollment period for the Marketplaces, more than
15.9 million women ages 18 to 64 were uninsured.
1
In addition to its early coverage improvements, the
Affordable Care Act made health coverage easier to obtain through the creation of the Health Insurance
Marketplaces and the expansion of Medicaid starting in 2014. The percentage of nonelderly women
(ages 18-64) who were uninsured fell slightly from 2010 to 2013, as public coverage, including
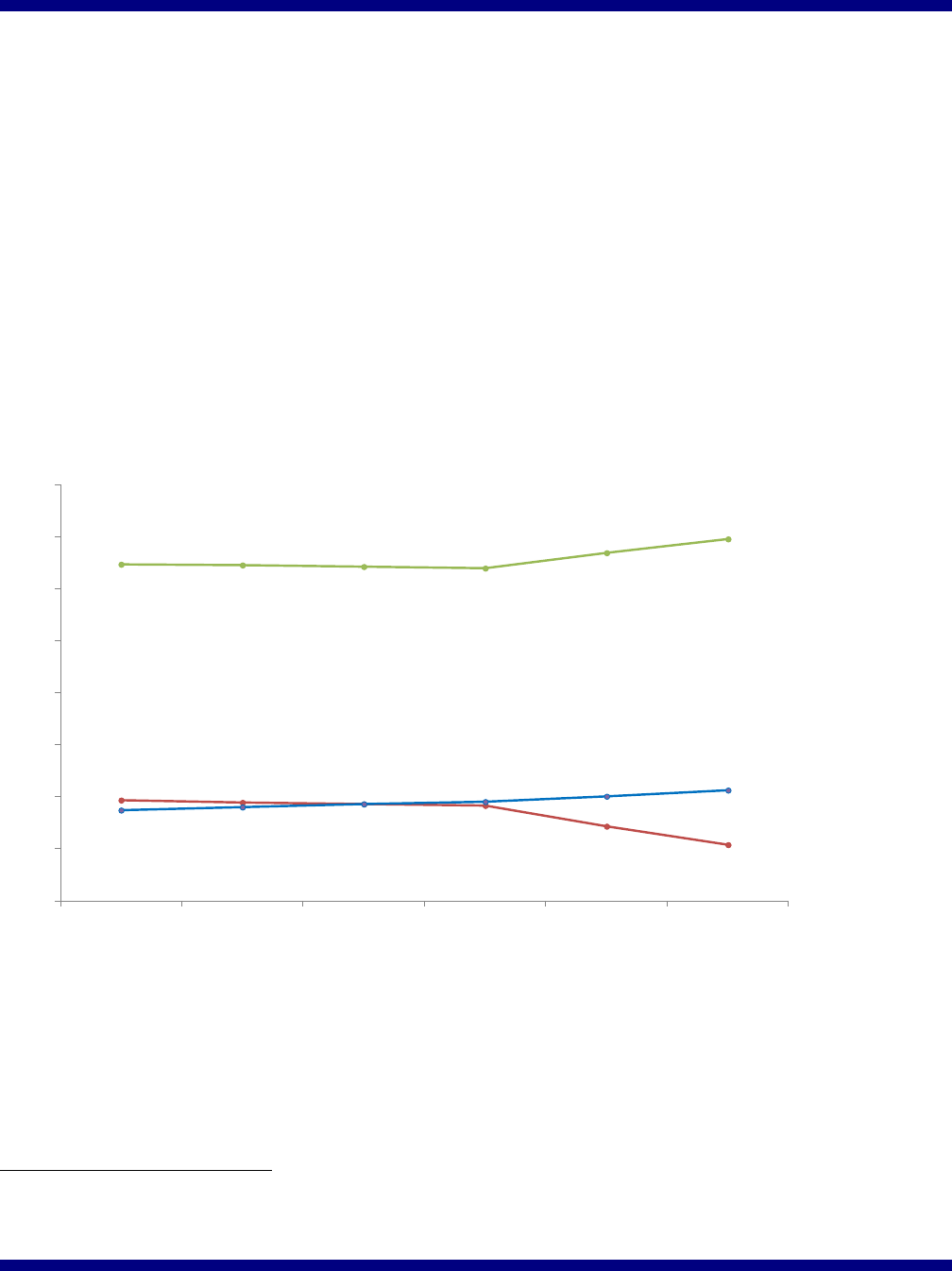
enrollment in Medicaid, increased; see Figure 1 below. Uninsured rates among women dropped more
sharply in 2014 and 2015, with increased private coverage, including Marketplace coverage, estimated
to account for most of the gains. Between 2010 and 2015, the uninsured rate among nonelderly women
decreased from 19.3 percent to 10.8 percent for a relative reduction of 44 percent, and the share with
private coverage increased from 64.7 percent to 69.6 percent.
Figure 1: Insurance Coverage among Women ages 18-64 (2010 to 2015)
19.3%
10.8%
64.7%
69.6%
17.4%
21.2%
0%
10%
20%
30%
40%
50%
60%
70%
80%
2010 2011 2012 2013 2014 2015
Private
Public
Uninsured
Notes: Ages 18-64. Sums may total more than 100% due to individuals reporting both public and private coverage.
Source: ASPE analysis of NHIS Early Release Program Data. U.S. Department of Health and Human Services, “Health
Insurance Coverage: Early Release of Quarterly Estimates from the National Health Interview Survey, January 2010-
December 2015,” Table 4. http://www.cdc.gov/nchs/data/nhis/earlyrelease/quarterly_estimates_2010_2015_q1234.pdf
1
Estimates of the “eligible uninsured” are ASPE tabulations of nonelderly (age 0-64) uninsured U.S. citizens and others
lawfully present from the 2012 American Community Survey Public Use Microdata Sample, adjusted to exclude estimated
undocumented persons based on imputations of immigrant legal status in ASPE's TRIM3 microsimulation model.
ASPE Issue Brief Page 4
ASPE Office of Health Policy
Health Insurance Marketplaces
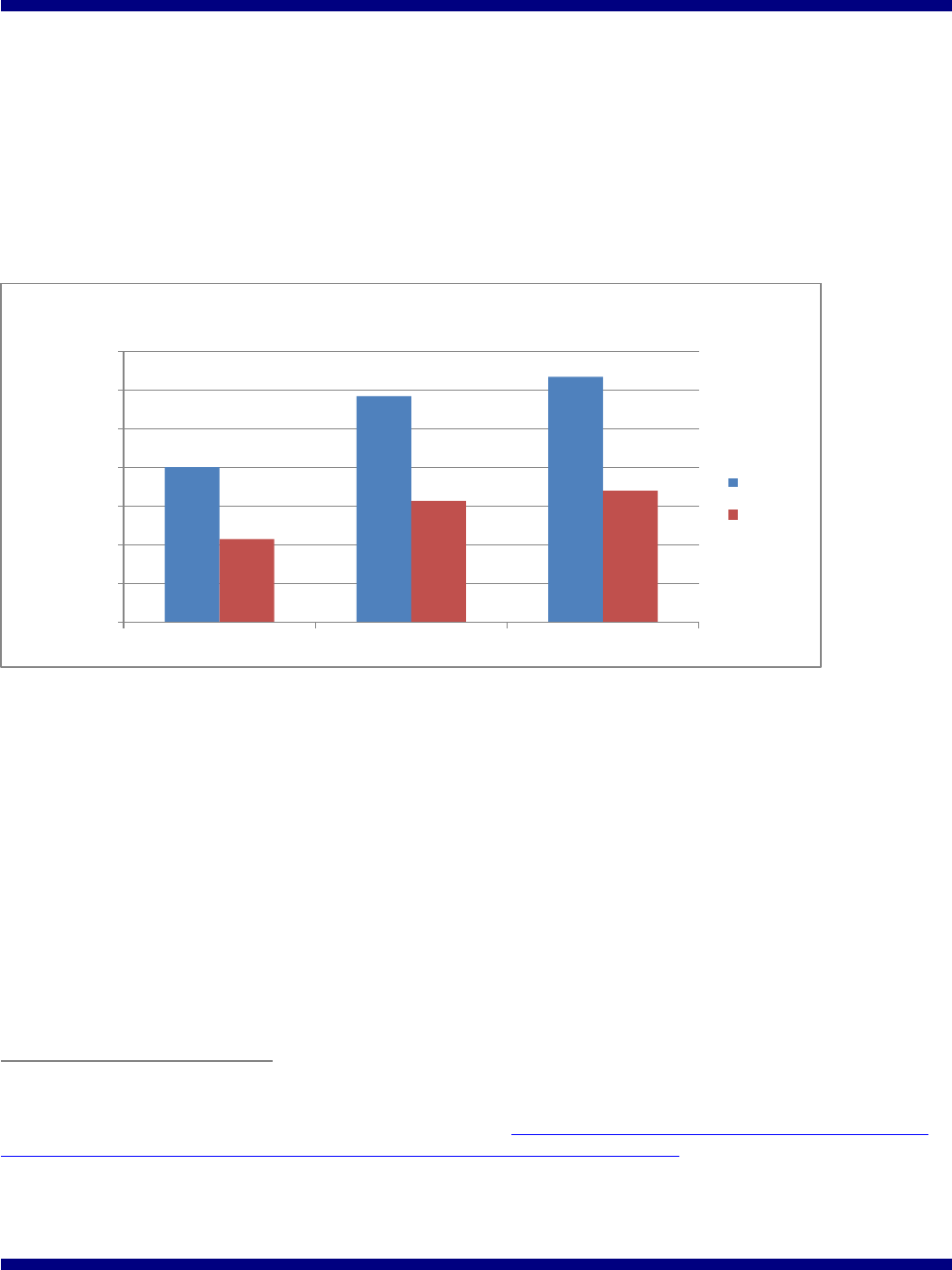
About 12.7 million Americans selected health plans for 2016 coverage through the Health Insurance
Marketplaces.
2
Of the total number who selected a Marketplace Plan during the 2016 Open Enrollment
period, 6.8 million (53.6 percent) are women and girls.
3
Figure 2 demonstrates the size of Marketplace
enrollment since 2014 and the number of women enrollees of all ages.
Figure 2: Marketplace Enrollment among Women and Girls (2014 to 2016)
Source: ASPE analysis of CMS Marketplace enrollment data.
Medicaid and CHIP
In 2014, Medicaid and the Children’s Health Insurance Program (CHIP) served 13 percent of women
ages 19 to 64 in the U.S.
4
The Affordable Care Act improved access to Medicaid coverage in several
notable ways. Medicaid’s expansion of eligibility to low-income adults with incomes below 138 percent
of the federal poverty level has expanded access to Medicaid coverage to millions of low-income
women in the 32 states that have adopted the expansion to date, and has the potential to benefit millions
more in the states that have not yet implemented the expansion. This group includes low-income parents
and pregnant women, who otherwise lose Medicaid coverage two months following delivery of their
newborn. Coverage through Medicaid increases access to quality health care and improves the financial
security for low-income individuals.
2
This amount does not include 400,000 people who signed up on the New York and Minnesota Marketplaces for coverage
through the Basic Health Program during this Open Enrollment. HHS Fact Sheet: About 12.7 million people nationwide are
signed up for coverage during Open Enrollment. February 4, 2016. http://www.hhs.gov/about/news/2016/02/04/fact-sheet-
about-127-million-people-nationwide-are-signed-coverage-during-open-enrollment.html#
3
Percentages are based on those who reported age/gender. The number of women presented in the graph is women and girls
of all ages. Additional information about 2016 Open Enrollment Period is available at https://aspe.hhs.gov/pdf-report/health-
insurance-marketplaces-2016-open-enrollment-period-final-enrollment-report.
4
ASPE analysis of 2014 NHIS public use data.
8,019,763
11,688,074
12,681,874
4,301,656
6,281,662
6,802,327
-
2,000,000
4,000,000
6,000,000
8,000,000
10,000,000
12,000,000
14,000,000
2014 2015 2016
Plan Selections in the Health Insurance Marketplace
Total
Women
ASPE Issue Brief Page 5
ASPE Office of Health Policy
The Affordable Care Act also amended the Medicaid statute to create a new optional eligibility group
such that states now have the option to provide family planning-related services and supplies to women
who previously only received coverage through section 1115 family planning demonstration projects.
To date, fourteen states have adopted the new family planning eligibility group.
II. Improving Affordability
Delayed or Forgone Care
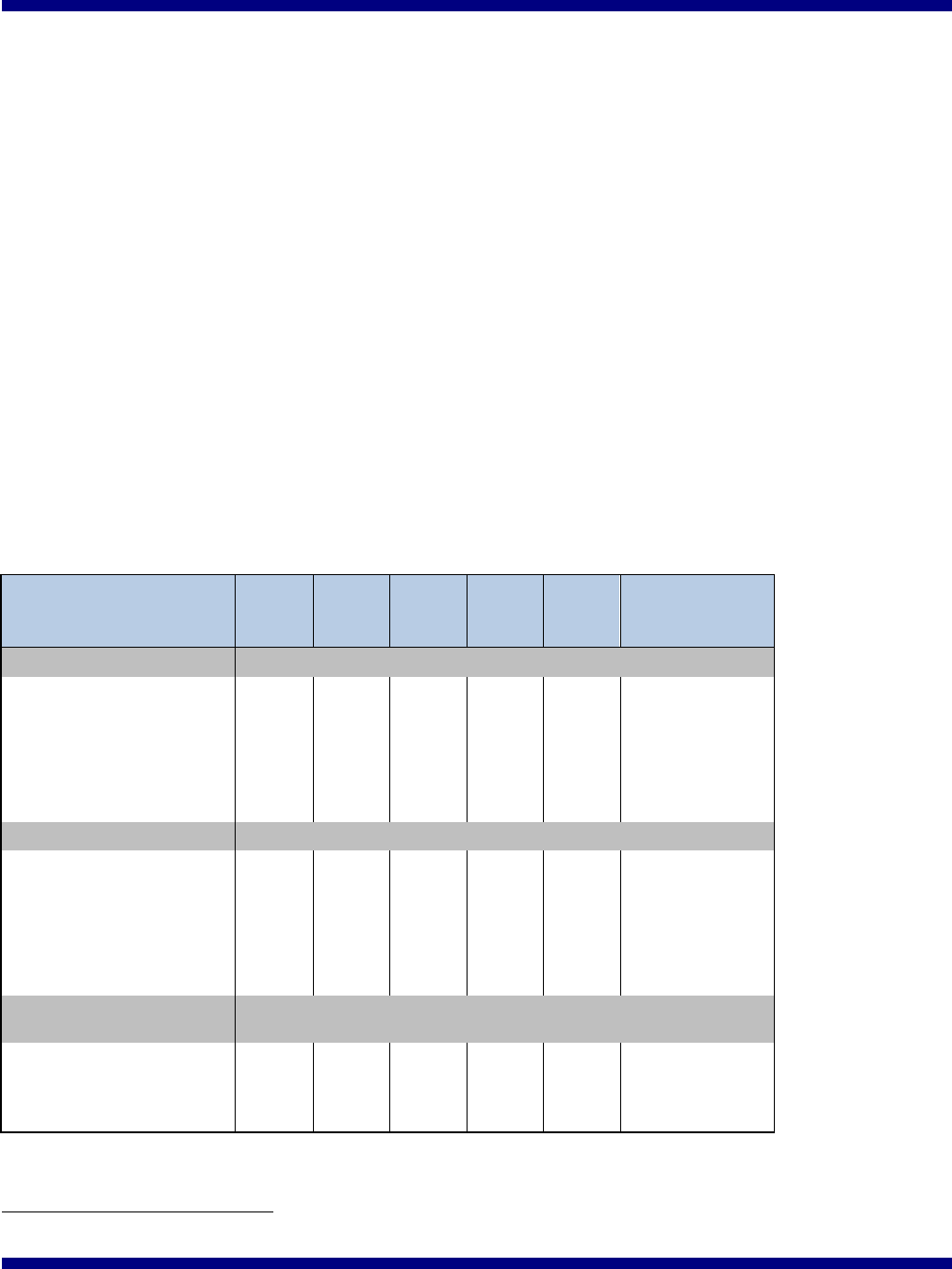
Since the implementation of the Affordable Care Act, fewer women report having delayed or forgone
care because of cost concerns. The proportion of young women (age 18-26) who reported delaying or
forgoing care dropped by 3.4 percentage points between 2010 and 2014; the proportion dropped by 3.5
percentage points among Black women, 4.1 percentage points among Hispanic women, and 3.0
percentage points among women with incomes at or below 400 percent of the federal poverty level
(Table 1).
5
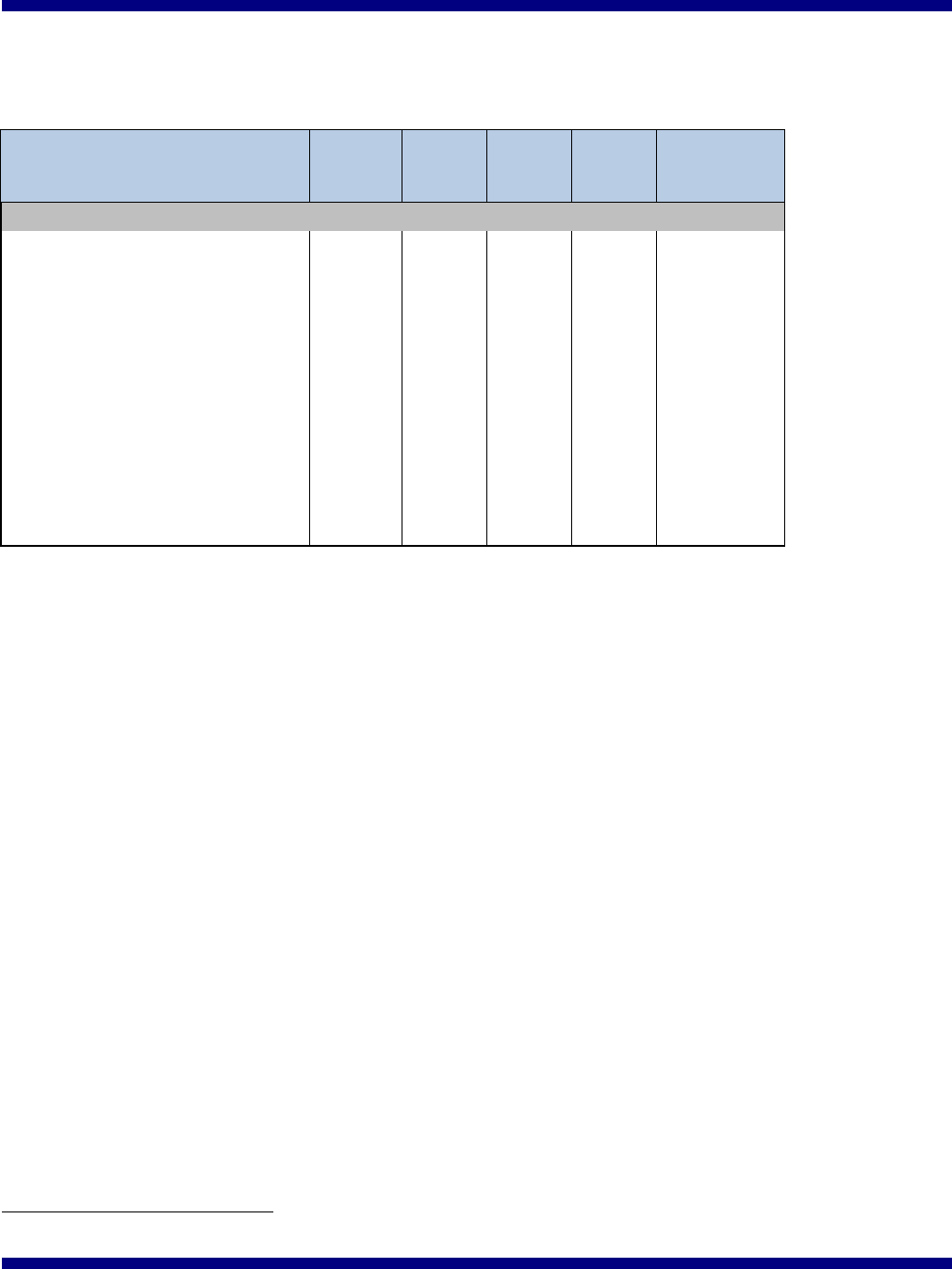
Table 1: Percentage of Women Who Had to Delay or Forgo
Care because of Cost (Weighted Percentages)
2010
2011
2012
2013
2014
Change
(percentage
points)
Age
18-26
15.5%
15.6%
13.3%
12.0%
12.1%
-3.4
27-39
16.6%
15.8%
15.7%
14.5%
13.9%
-2.7
40-49
16.6%
18.6%
16.7%
14.9%
14.1%
-2.5
50-64
17.2%
16.2%
16.4%
15.6%
14.1%
-3.1
65+
5.4%
5.2%
4.6%
4.6%
5.0%
-0.4
Race/ethnicity
White, non-Hispanic
13.7%
13.5%
12.9%
11.8%
11.6%
-2.1
Black, non-Hispanic
18.6%
18.3%
15.9%
16.8%
15.1%
-3.5
Hispanic
17.0%
17.2%
16.2%
14.0%
12.9%
-4.1
Asian/PI
6.8%
7.0%
7.0%
6.0%
5.5%
-1.3
Other
12.3%
14.7%
12.0%
11.5%
9.1%
-3.2
Income as % of federal
poverty level
≤400%
19.7%
19.9%
18.6%
17.5%
16.7%
-3.0
>400%
7.4%
5.9%
5.8%
4.9%
4.8%
-2.6
Missing
9.0%
10.4%
9.6%
9.5%
5.7%
-3.3
Source: ASPE analysis of NHIS 2010-2014.
5
All four trends are statistically significant (p-value<0.05).

ASPE Issue Brief Page 6
ASPE Office of Health Policy
Medicaid Expansion and Hospital Care
A particular point of financial vulnerability for women is the cost of hospital care, which is often
expensive and may not be planned. In states that expanded Medicaid under the Affordable Care Act,
women were less likely to be left uninsured during a hospitalization than in states that did not expand
Medicaid.
6
The proportion of inpatient hospital discharges attributable to uninsured women in states that
expanded Medicaid dropped by 3.3 percentage points from 7.1 percent in 2010 to 3.8 percent in 2014; in
contrast, in non-expansion states, the proportion of inpatient discharges attributable to uninsured women
decreased by only 1.7 percentage points from 8.0 percent to 6.3 percent.
7
Put another way, the number
of uninsured hospitalizations in Medicaid expansion states decreased by 50.5 percent (from 381,776 in
2010 to 188,798 in 2014), while the number of uninsured hospitalizations in non-expansion states
decreased by only 4.0 percent (from 415,438 in 2010 to 398,745 in 2014).
8
This coverage trend
demonstrates the financial protections created by the Affordable Care Act, and Medicaid expansion in
particular, and helps explain why hospitals in Medicaid expansion states also have more significant
reductions in uncompensated care since passage of the Affordable Care Act than hospitals in non-
expansion states.
9
Medicare Prescription Drugs
Prior to the Affordable Care Act, Medicare Part D beneficiaries experienced a coverage gap in their
prescription drug coverage, termed the “donut hole”. The Affordable Care Act closes the donut hole
over several years until it is completely closed in 2020. Since this Affordable Care Act provision went
into effect in 2010 through 2015, beneficiaries with Medicare prescription drug coverage have saved
more than $20 billion on prescription drugs -- including savings of $11 billion for the more than 6
million women with Medicare Part D.
10
Concurrently, women with Medicare Part D note an
improvement in affordability, with a 3.8 percentage point decline in the proportion of women saying
they could not afford prescription medication in the past 12 months (Table 2).
11
6
Hu, L, Kaestner, R, Mazumder, B, Miller, S, Wong, A. “The Effect of the Patient Protection and Affordable Care Act
Medicaid Expansions on Financial Well-Being,” National Bureau of Economic Research, Working Paper 22170, April 2016.
http://www.nber.org/papers/w22170.
7
AHRQ analysis of 2010 and 2014 Healthcare Cost and Utilization Project (HCUP), State Inpatient Databases (SID) data.
For this analysis, Expansion States include AR, AZ, CA, CO, CT, HI, IA, IL, KY, MD, MI, MN, NJ, NM, NV, NY, OH, OR,
RI, VT, WA, WV (n=22); Nonexpansion States include FL, GA, IN, KS, LA, MO, MT, NC, NE, OK, PA, SC, SD, TN, TX,
VA, WI, WY (n=18). Four States (IN, LA, MT, PA) that expanded their Medicaid programs in 2015 or 2016, are considered
as Nonexpansion States for this analysis.
8
Agency for Healthcare Research and Quality (AHRQ) analysis of Healthcare Cost and Utilization Project (HCUP), State
Inpatient Databases (SID), 2010 and 2014.
9
HHS, Office of the Assistant Secretary for Planning and Evaluation, 2015. ASPE Issue Brief: Insurance Expansion,
Hospital Uncompensated Care, and the Affordable Care Act. https://aspe.hhs.gov/pdf-report/insurance-expansion-hospital-
uncompensated-care-and-affordable-care-act
10
ASPE estimated the number of women who had Medicare Part D savings during 2010-2015 based on CMS’s estimated
total number of beneficiaries with Part D savings (https://www.cms.gov/Newsroom/MediaReleaseDatabase/Press-
releases/2016-Press-releases-items/2016-02-08.html) and the ratio of female to total non-Low Income Subsidy beneficiaries
generated from Medicare Prescription Drug Event (PDE) data.
11
This trend is statistically significant (p-value<0.001).
ASPE Issue Brief Page 7
ASPE Office of Health Policy
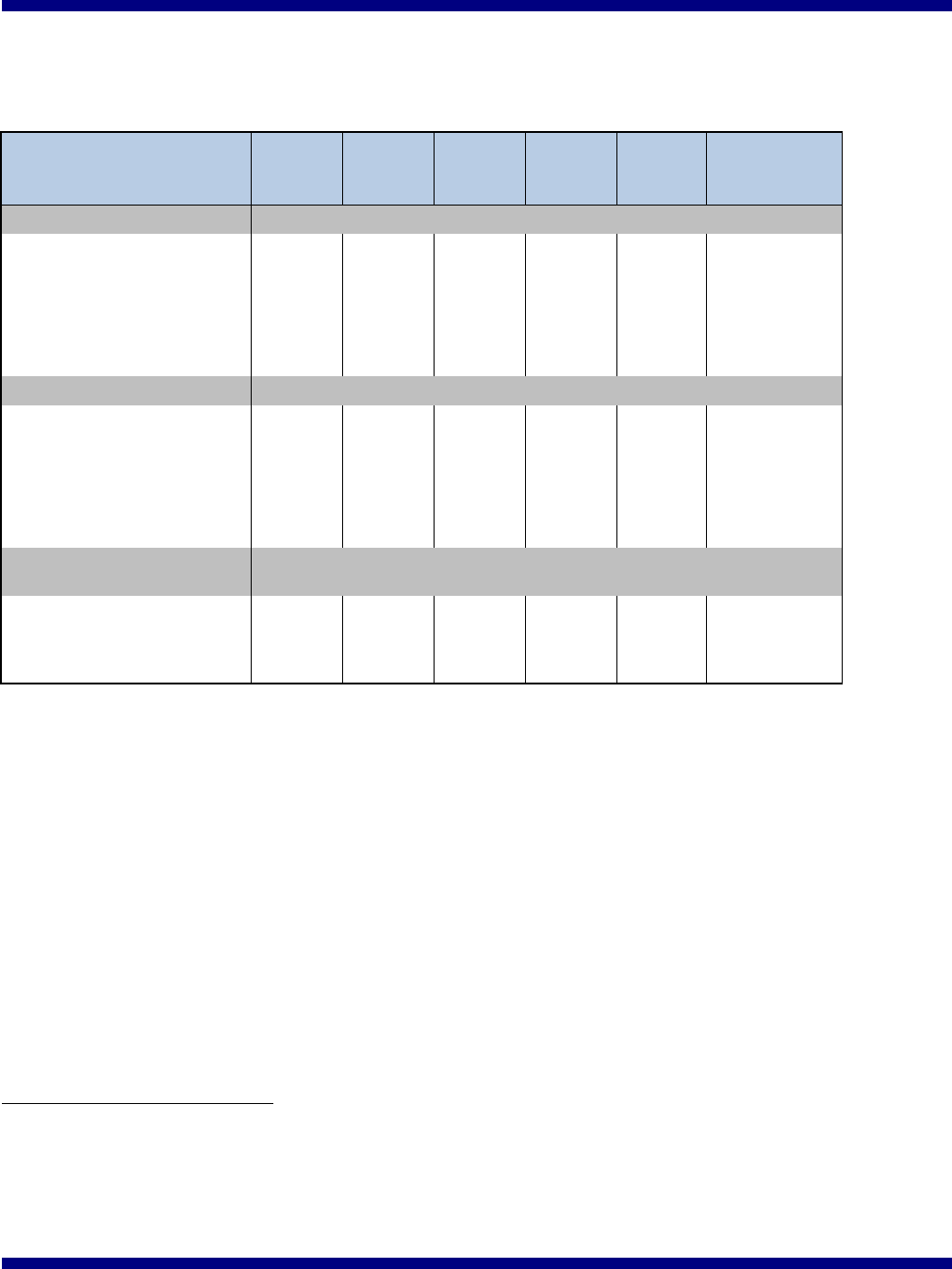
Table 2: Trends in Prescription Drug Affordability for Women Medicare Part D Beneficiaries,
Ages 65+, Unadjusted
2011
2012
2013
2014
Change
(percentage
points)
Prescription Drug Affordability
Skipped medication doses
6.8%
5.1%
5.1%
4.8%
-2.0
Took less Medicine
7.6%
5.1%
5.3%
4.8%
-2.8
Delayed filling a prescription to
save money
8.9%
6.7%
7.1%
6.5%
-2.4
Any limitation in prescription
drug affordability (Any Above)
10.8%
7.7%
8.5%
7.8%
-3.0
Asked your doctor for a lower
cost medication
25.6%
24.3%
21.3%
21.2%
-4.4
Bought prescription drugs from
another country
2.1%
1.1%
1.6%
1.4%
-0.7
Could not afford prescription
medication, past 12 months
10.2%
6.8%
7.2%
6.4%
-3.8
Source: ASPE Analysis of NHIS 2011-2014.
III. Improving Quality of Coverage and Health Care
Preventive Health Services
The Affordable Care Act requires most private health insurance plans to cover preventive benefits
recommended by the U.S. Preventive Services Task Force and the Advisory Committee on
Immunization Practices without cost-sharing. For example, since September 23, 2010, non-
grandfathered plans subject to this requirement must cover recommended services including
mammograms, screenings for cervical cancer, tobacco cessation services, and flu and pneumonia shots
without cost-sharing.
12
The Affordable Care Act also enhanced Medicare coverage of recommended
preventive services, including screening mammograms, by waiving cost-sharing (coinsurance or
deductible) that would otherwise apply. In addition, Medicare beneficiaries can now get a free Annual
Wellness Visit. The Affordable Care Act aligned Medicaid coverage for the newly eligible with that
offered by private insurance by covering the ten essential health benefits through alternative benefit plan
(ABP) coverage. This means that women covered through Medicaid expansion have access to
preventive services and other coverage similar to that offered in the private insurance market, including
access to all eighteen Food and Drug Administration approved contraceptives.
12
HHS. Preventive care benefits: Preventive health services for adults. https://www.healthcare.gov/preventive-care-benefits/
ASPE Issue Brief Page 8
ASPE Office of Health Policy
The Affordable Care Act also included a provision that took effect beginning on August 1, 2012,
requiring most insurers to cover certain additional recommended preventive health services – established
under the Women’s Preventive Services Guidelines
13
– without charging a copay, coinsurance, or
deductible. Millions have gained expanded coverage of these services including contraceptive
education, counseling, methods, and services; well-woman visits; sexually-transmitted infection
counseling; Human Immunodeficiency Virus (HIV) screening and counseling; screening for gestational
diabetes, breastfeeding support, supplies, and counseling; and domestic violence screening and
counseling – all without cost sharing.
14
It is estimated that 55.6 million women with private insurance
are guaranteed coverage of recommended preventive services with no out-of-pocket costs.
15
Not having
to face the barrier of cost sharing for women’s preventive services means greater access to
recommended screenings and other services that can help protect women’s health, and access to family
planning services to help women space their pregnancies to promote optimal birth outcomes.
16
Usual Source of Care
As shown in Table 3, there have been gains in the percentage of women with a usual source of care,
particularly among young women (a 5.2 percentage point increase between 2010 and 2014), Black
women (a 5.1 percentage point increase), Hispanic women (a 6.5 percentage point increase), and women
with incomes at or below 400 percent of the federal poverty level (a 3.8 percentage point increase).
17
13
The Health Resources and Services Administration awarded a five-year cooperative agreement to the American College of
Obstetricians and Gynecologists to develop a collaborative process to review and recommend updates to the guidelines.
http://www.hrsa.gov/womensguidelines/updatingwomensguidelines.html
14
HRSA. Women’s Preventive Services Guidelines. http://www.hrsa.gov/womensguidelines/
15
HHS, Office of the Assistant Secretary for Planning and Evaluation, 2015. ASPE Data Point: The Affordable Care Act is
Improving Access to Preventive Services for Millions of Americans. https://aspe.hhs.gov/pdf-document/affordable-care-act-
improving-access-preventive-services-millions-americans
16
Institute of Medicine, 2011. Clinical Preventive Services for Women: Closing the Gaps.
http://iom.nationalacademies.org/Reports/2011/Clinical-Preventive-Services-for-Women-Closing-the-
Gaps.aspx#sthash.350trMBF.dpuf
17
All four trends are statistically significant (p<0.01).
ASPE Issue Brief Page 9
ASPE Office of Health Policy
Table 3: Percentage of Women with a Usual Source of Care
(weighted percentages)
2010
2011
2012
2013
2014
Change
(percentage
points)
Age
18-26
75.3%
77.7%
75.1%
75.5%
80.5%
5.2
27-39
81.1%
82.2%
81.3%
81.0%
83.8%
2.7
40-49
87.2%
88.1%
85.4%
87.7%
89.5%
2.3
50-64
89.4%
91.5%
89.7%
91.4%
91.9%
2.5
65+
95.8%
96.0%
95.9%
96.3%
96.7%
0.9
Race/ethnicity
White, non-Hispanic
89.1%
90.3%
88.7%
89.3%
91.1%
2.0
Black, non-Hispanic
83.0%
85.0%
83.9%
86.7%
88.1%
5.1
Hispanic
74.3%
76.3%
76.5%
77.6%
80.8%
6.5
Asian/Pacific Islander
86.8%
86.4%
84.3%
85.7%
87.4%
0.6
Other
82.0%
84.6%
82.3%
84.3%
87.5%
5.5
Income as % of federal
poverty level
≤400%
82.2%
83.1%
82.7%
82.8%
86.0%
3.8
>400%
92.5%
94.9%
92.5%
93.9%
93.8%
1.3
Missing
88.0%
89.1%
84.8%
88.2%
91.2%
3.2
Source: ASPE analysis of NHIS 2010-2014.
Maternity Care
The Affordable Care Act also funded the Strong Start for Mothers and Newborns Initiative, a
collaborative effort by the Centers for Medicare & Medicaid Services (CMS), the Health Resources and
Services Administration, and the Administration on Children and Families, to reduce preterm births and
improve health outcomes for newborns and pregnant women.
18
In the first stage of this initiative, sites
participating in the Partnership for Patients identified and disseminated best practices to reduce the
number of early elective deliveries among pregnant women. Between 2010 and 2013, there was a 70.4
percent reduction in early elective deliveries among participating hospitals,
19
and, as of May 2014, more
than 25,000 early elective deliveries were prevented.
20
,
21
Close to 200 sites are currently participating in
an initiative to test and evaluate enhanced prenatal care interventions for women enrolled in Medicaid or
CHIP who are at risk for having a preterm birth.
18
HHS, Centers for Medicare & Medicaid Services. Strong Start for Mothers and Newborns Initiative: General Information.
Accessed at http://innovation.cms.gov/initiatives/strong-start/
19
CMS Fact Sheet (July 30, 2015). https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2015-Fact-sheets-
items/2015-07-30-3.html
20
March of Dimes. 2015 Annual Report. http://www.marchofdimes.org/materials/2015-annual-report.pdf
21
HHS Office on Women’s Health. 2015 Report to Congress: HHS Activities to Improve Women’s Health.

ASPE Issue Brief Page 10
ASPE Office of Health Policy
As mentioned above, in addition to funding the Strong Start for Mothers and Newborns Initiative, the
Affordable Care Act amended the Medicaid program by requiring states to cover counseling and
pharmacotherapy for cessation of tobacco use by pregnant women with no cost sharing. This new
mandatory Medicaid benefit aligns with the services recommended by the U.S. Preventive Services Task
Force.
IV. Conclusion
Numerous provisions of the Affordable Care Act address the unique health care needs of women, and
the resulting impacts are clear through improvements in access, affordability, and quality of coverage
and care. As implementation of the Affordable Care Act continues, provisions designed to strengthen
preventive care, ensure the availability of affordable insurance coverage options, and improve health
care delivery for all Americans will continue to promote better health outcomes for women.
