www.lao.ca.gov
2022-23 BUDGET
1
Summary
This brief focuses on access to health insurance coverage and the affordability of health care
costs. We assess various Governor’s proposals intended to improve health care access and/or
affordability, discuss options to improve affordability of health plans purchased through Covered
California, and highlight some key access and affordability challenges that remain to address.
Expand Full-Scope Medi-Cal Coverage to All Remaining Income-Eligible Undocumented
Populations. Building on previously approved expansions, the Governor proposes to expand
full-scope Medi-Cal coverage to income-eligible, undocumented residents aged 26 through 49
beginning no sooner than January 1, 2024. We discuss options to provide coverage earlier and
ensure certain young adults do not lose coverage prior to January 1, 2024.
Reduce Medi-Cal Premiums to Zero Cost. Certain individuals who are otherwise not
income-eligible for Medi-Cal can enroll if they pay premiums. The Governor proposes reducing
these premiums to zero. While we agree with the policy basis for this proposal, additional
information is needed to determine if it should be approved as is or with modifications.
Establish Office of Health Care Affordability. The Governor re-proposes to create the
Office of Health Care Affordability—intended to control rising overall health care costs. We find
that, in concept, the proposal to create this new office is reasonable, but ambitious. Continued
monitoring would be necessary to ensure the office achieves its goals. As such, we recommend
the Legislature consider (1) whether any adjustments are needed to the proposed trailer bill
language creating the office and (2) establishing a process for legislative oversight.
Reduce the Cost of Insulin Through State Partnership. Chapter 207 of 2020 (SB 852, Pan)
directed the state to enter into partnerships to produce and distribute generic prescription drugs
to improve affordability. The Governor announced a future proposal to manufacture insulin.
We recommend withholding approval until more information is provided to ensure the proposal
meets SB 852’s criteria for viability and other factors.
Options to Improve Covered California Affordability. At the direction of the Legislature,
Covered California developed options for cost-sharing reductions to improve the affordability of
plans offered on its exchange. We discuss various issues for the Legislature to consider when
deciding on any actions related to these options.
Various Access and Affordability Issues Remain. In the final section, we discuss various
access and affordability issues that will remain even if the Legislature approves the Governor’s
proposals and addresses affordability of Covered California health plans.
GABRIEL PETEK | LEGISLATIVE ANALYST
FEBRUARY 2022
The 2022-23 Budget:
Health Care Access and Affordability

LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
2
INTRODUCTION
Health Care Access and Affordability.
Health care access and affordability are a challenge
for many Californians. Notably, roughly 3.2 million
Californians lack access to comprehensive
health insurance. Even those who do have health
insurance can struggle with health care costs that
can consume a large portion of their annual income.
These challenges have prompted recent actions
by the Legislature and a number of additional
proposals in the Governor’s budget as well as other
issues for the Legislature to consider during the
current budget cycle.
Report Focuses on Issues Related to Health
Insurance Coverage and Health Care Costs.
While there are a broad range of issues impacting
both the affordability and access to quality health
care services, this report focuses on access to
health insurance coverage and the affordability
of health care costs Californians face. In this
context, we first provide an assessment of various
Governor’s budget proposals intended to improve
health care access and/or affordability. (We provide
an assessment of proposals potentially affecting
access through other means, such as by increasing
Medi-Cal provider payment levels, in other budget
publications.) We then discuss issues for the
Legislature to consider as it evaluates options
to improve the affordability of health insurance
coverage offered on the state’s health benefit
exchange—Covered California. Finally, we conclude
with a brief discussion of some key access and
affordability challenges that likely would remain
even if the Legislature approves the Governor’s
proposals and takes action to improve affordability
within Covered California.
BACKGROUND
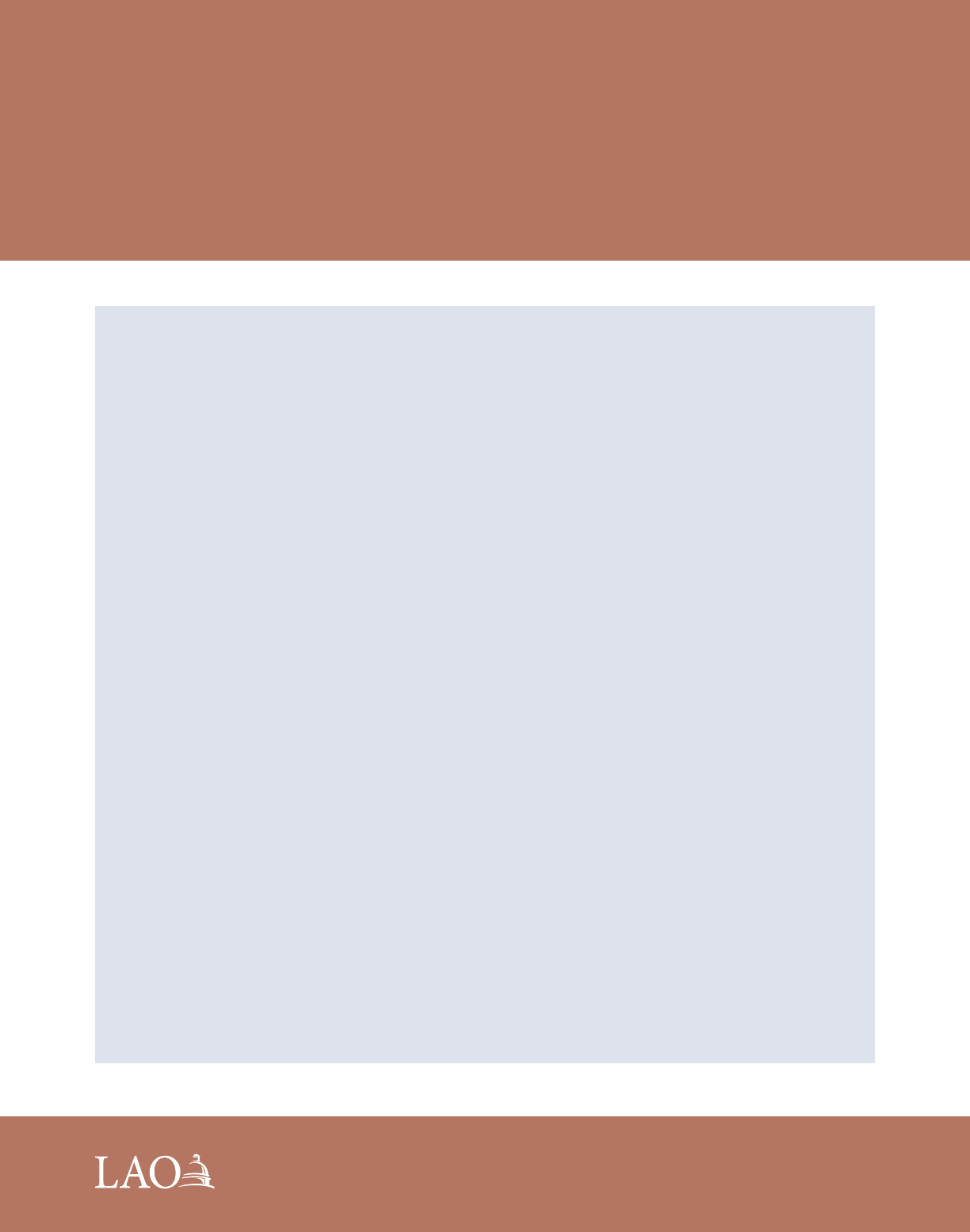
Most Californians Have Health Insurance…
As shown in Figure 1, we estimate that most
Californians—92 percent—have health insurance
coverage. (Compared with other states, California’s
rate of insurance is roughly in the middle—some
states have higher rates of insurance, while others
have lower rates of insurance.) Employer-sponsored
insurance is the most common source of coverage.
Major public health insurance programs, including
Medi-Cal, the state’s Medicaid program which
covers low-income people, and Medicare, the
federal program that primarily provides health
coverage to the elderly, also cover large portions of
the state’s residents.
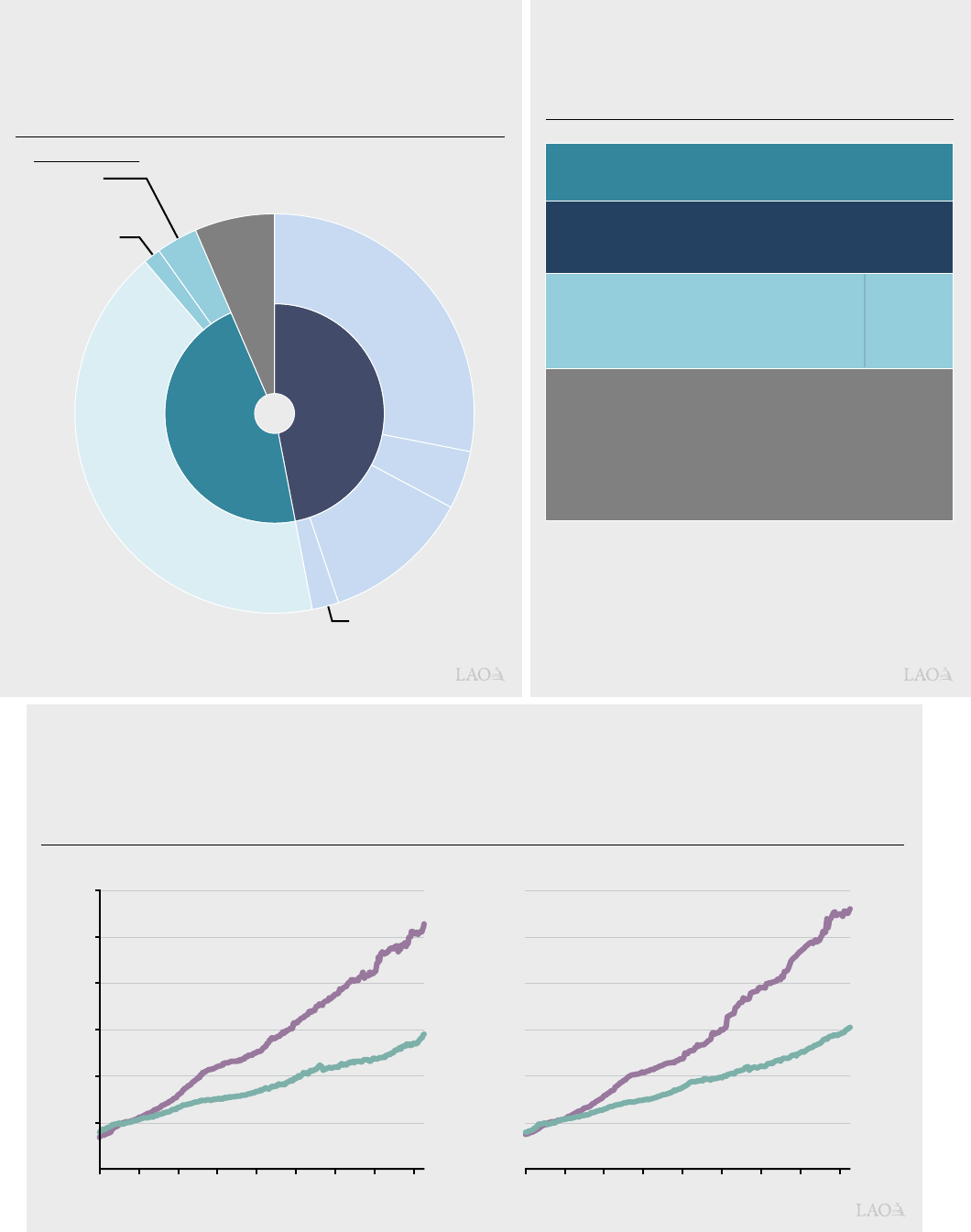
…But an Estimated 3.2 Million Californians
Lack Comprehensive Insurance. While most
Californians have comprehensive health insurance,
an estimated roughly 3.2 million people (about
8 percent) in the state lack such coverage in
2022—including people who are uninsured or
have “restricted-scope” Medi-Cal that only covers
emergency- and pregnancy-related health services.
However, these figures do not reflect a previously
approved expansion of comprehensive Medi-Cal
coverage to undocumented residents who are
50 or older which will go into effect in May 2022.
In addition, the estimate does not reflect impacts
of a federal policy change regarding Medi-Cal
enrollment during the COVID-19 national public
health emergency (which likely increased insurance
coverage). As shown in Figure 2, the majority
of uninsured Californians are undocumented
residents, followed by individuals who are eligible
for but not enrolled in insurance from a variety
of sources.
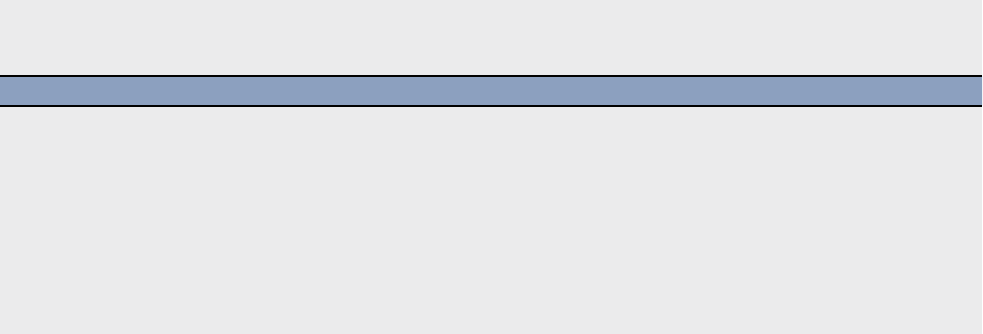
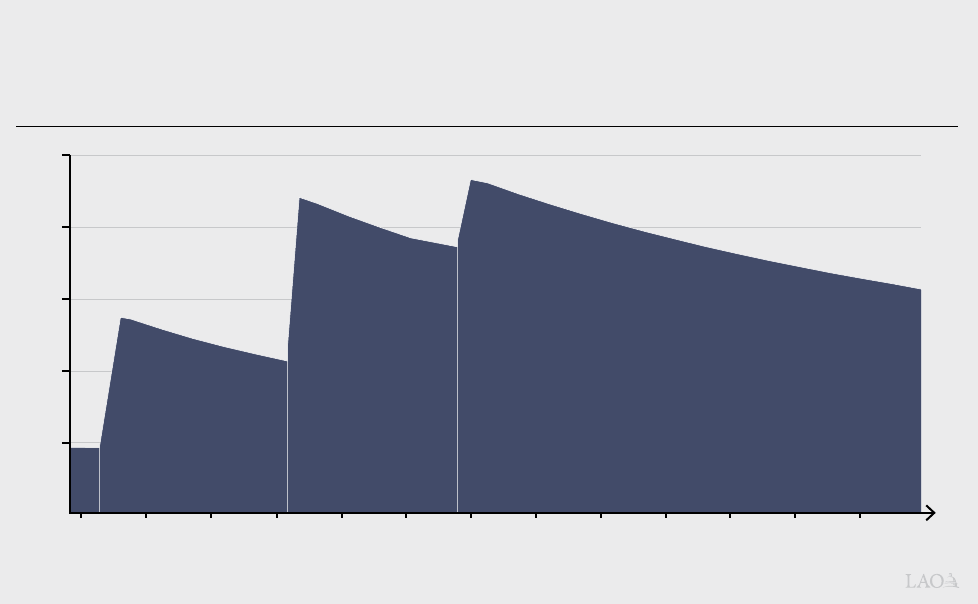
Affordability of Health Care Remains a
Challenge. Over the last several decades, health
care costs have grown significantly. To a significant
degree, this cost growth has been driven by growth
in health care prices. As Figure 3 shows, medical
inflation in major California metro areas has far
outpaced inflation for other goods and services
in recent decades, reducing what Californians
can afford to spend on these other goods and
services. While other expenditures such as
housing have a greater impact on California’s
cost of living, Californians need to balance
health care costs with these other expenditures.
www.lao.ca.gov
2022-23 BUDGET
3
a
Documented residents who can purchase plans through Covered California but
do not meet certain federal requirements to qualify for federal subsidies.
b
This number does not reflect a previously-authorized expansion of full-scope
Medi-Cal benefits to undocumented residents who are 50 or older, which will be
implemented in May 2022.
Source: UC Berkeley, UC Los Angeles; California Simulation of Insurance
Markets, Version 3.0.
Figure 2
Roughly 3.2 Million Californians
Lack Health Insurance in 2022
Eligible for Employer-Sponsored Coverage
480,000
Eligible for Medi-Cal
610,000
With
Subsidies
630,000
Undocumented
b
1,270,000
Without
Subsidies
a
170,000
Eligible for Covered California
Figure 1
Most Californians Have Health Insurance,
Obtained From a Variety of Sources
2020 Estimated
a
Remaining roughly 400,000 purchased coverage “off exchange.”
Note: Estimates reflect LAO adjustments to California Health Interview Survey 2020 data.
Private
Insurance
Public
Insurance
Employer-
Sponsored
Insurance
Uninsured
Medi-Cal
Medicare
Other Public
Insurance
Medicare
and Medi-Cal
Unsubsidized
0.6 Million
(About 186,000
on Covered
California)
a
Subsidized
1.3 Million
(All on Covered
California)
Individual Market
Source: LAO estimate based on Bureau of Labor Statistics Consumer Price Index for all urban consumers.
Figure 3
Medical Prices Have Grown Significantly Faster
Than Nonmedical Prices in Major California Metro Areas
Consumer Price Index
Medical
Inflation
Nonmedical
Inflation
100
200
300
400
500
600
1980 1985 1990 1995 2000 2005 2010 2015 2020 1980 1985 1990 1995 2000 2005 2010 2015 2020
Greater Los Angeles
(Los Angeles, Long Beach, and Anaheim)
Medical
Inflation
Nonmedical
Inflation
Bay Area
(San Francisco, Oakland, and Hayward)

LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
4
According to a survey conducted between
November 2020 and January 2021, roughly
82 percent of Californians stated that it was either
very or extremely important for the Legislature and
Governor to make health care more affordable.
In the same survey, roughly half of Californians
decided to delay, skip, or reduce their utilization of
health care in the prior 12 months due to costs. Of
those who made such decisions, 41 percent stated
that the steps they took to reduce costs had a
negative impact on their health.
GOVERNOR’S PROPOSALS TO IMPROVE
HEALTH CARE ACCESS AND AFFORDABILITY
EXPAND FULL-SCOPE MEDI-CAL
COVERAGE TO REMAINING
UNDOCUMENTED POPULATIONS
Background
Historically, Undocumented Residents Were
Eligible Only for Restricted-Scope Medi-Cal
Coverage. Medi-Cal eligibility depends on a
number of individual and household characteristics,
including, for example, income, age, and
immigration status. Historically, income-eligible
citizens and immigrants with documented status
generally have qualified for comprehensive, or
full-scope, Medi-Cal coverage, while otherwise
income-eligible undocumented immigrants have
not qualified for full-scope Medi-Cal coverage.
Up until recently, all undocumented residents
who met the income criteria for Medi-Cal have
been eligible only for restricted-scope Medi-Cal
coverage, which only covers emergency- and
pregnancy-related health care services. The federal
government pays for a portion of undocumented
immigrants’ restricted-scope Medi-Cal
services according to standard federal-state
cost-sharing rules.
State Has Expanded Full-Scope Medi-Cal
Coverage to Many, but Not All, Otherwise
Income-Eligible Undocumented Residents.
The state has taken steps to expand eligibility
for full-scope Medi-Cal coverage to otherwise
eligible undocumented residents in various
age groups. First, in 2016, the state expanded
full-scope Medi-Cal coverage to otherwise eligible
undocumented children from birth through
age 18. Then, in 2020, the state expanded
full-scope Medi-Cal coverage to otherwise eligible
undocumented young adults ages 19 through 25.
Most recently, as part of the 2021-22 budget
package, the state passed legislation to expand
eligibility to undocumented residents who are 50 or
older beginning May 1, 2022. The costs of these
expansions are paid almost entirely by the state
because the federal government only shares in the
cost of restricted-scope services. Accounting for
these recently enacted expansions, undocumented
adults who are between the ages of 26 and 49,
inclusive, are the remaining undocumented
population eligible for only restricted-scope
Medi-Cal. Once the 50-and-older expansion is fully
implemented, we estimate that a little over 1 million
undocumented immigrants will have full-scope
Medi-Cal coverage.
Proposal
The Governor proposes to expand full-scope
Medi-Cal coverage to income-eligible
undocumented residents aged 26 through 49
beginning no sooner than January 1, 2024. Due to
past expansions, this proposal would effectively
provide universal access to Medi-Cal regardless of
immigration status. The administration estimates
that in 2023-24, the first year of the expansion,
714,000 undocumented residents between the
ages of 26 through 49 would enroll in Medi-Cal
and that this would increase to 764,000 residents
at full implementation. Due to the proposed
implementation date, there is no budgetary impact
in 2022-23. The administration estimates that the
expansion would result in costs of $613.5 million
General Fund ($819.3 million total funds) in 2023-24
and $2.2 billion General Fund ($2.7 billion total
www.lao.ca.gov
2022-23 BUDGET
5
funds) annually at full implementation. The growth
in projected spending primarily is due to annualizing
half-year costs in 2023-24 and projected gradual
increases in the uptake of In-Home Supportive
Services among beneficiaries, along with gradual
increases in caseload.
Assessment
Proposal Consistent With Statutory Goals
and Recent Legislation. The Governor’s
proposal is consistent with past legislative efforts
to expand Medi-Cal coverage to younger and
older undocumented residents. It also further the
goals established in Chapter 34 of 2018 (AB 1810,
Committee on Budget) which, among other goals,
declared an intent that all Californians (1) receive
high-quality health care regardless of various
factors including age and immigration status and
(2) have access to affordable health coverage.
Proposal Would Significantly Reduce Number
of Californians Who Lack Comprehensive
Insurance. If the administration’s caseload
assumptions are correct, this proposal would
substantially reduce the number of Californian’s
who do not have access to comprehensive
health insurance. Using the administration’s
assumptions for this proposal, and assuming that
235,000 undocumented residents who are 50 or
older will enroll in Medi-Cal once they are eligible
this May under previously enacted legislation, we
estimate that the number of Californians who lack
comprehensive health insurance would go down
to about 2.2 million people following the proposal’s
full implementation, which is roughly 1 million lower
than the current level of about 3.2 million people.
Continuing to Evaluate Administration’s
Caseload and Cost Estimates. Due to the
availability of data at the time of this analysis, we
have not yet evaluated the reasonableness of the
administration’s estimates of the caseload and
cost impacts of this proposal. Any estimate of
expansion cost and caseload, however, is subject
to considerable uncertainty. For example, while
restricted-scope enrollees generally automatically
would shift over to full-scope coverage once
eligible, how many of the individuals who are not
currently enrolled in restricted-scope coverage
would choose to enroll in full-scope coverage once
eligible is unclear. In addition, average costs for this
caseload could be significantly different than the
average costs for current full-scope enrollees due
to differences in their health needs. For example,
research on the health of the U.S. and California
populations shows that immigrants, including
undocumented immigrants, have lower disability
rates than other residents. To the extent this is
true for the proposed expansion population, their
average per-enrollee costs could be significantly
lower than existing full-scope enrollees. This is
because Medi-Cal enrollees with disabilities tend
to have health care costs that are two to ten times
higher on a per-enrollee basis than other enrollees.
Extended Time Frame Relative to Past
Expansions Impacts Access to Coverage.
As currently structured, this expansion would
occur no sooner than a year and a half following its
approval (provided it is approved). In comparison,
past expansions were implemented within a year of
being approved. Adopting a similar implementation
time frame as past expansions for all or part
of this remaining age group would accelerate
implementation and could improve access to
health care sooner. Moreover, the extended
implementation time frame could result in some
young adults losing coverage while waiting for
the proposal to be implemented. Currently, the
potential number of young adults who could lose
full-scope coverage prior to January 1, 2024 is
particularly large because many young adults
who otherwise would have aged out of full-scope
Medi-Cal (upon turning 26 years of age) have
been able to keep their benefits as a result of a
federal policy that effectively prevented eligibility
terminations except in limited circumstances during
the COVID-19 national public health emergency.
(For more information on this federal policy and
its impacts on the Medi-Cal caseload, please
see our recent publication, The 2022-23 Budget:
Analysis of the Medi-Cal Budget.) While there is
some uncertainty regarding the number of young
adults who would lose full-scope coverage once
the public health emergency ends, we estimate that
upwards of 40,000 undocumented young adults
could lose full-scope coverage between the end
of the public health emergency until they would
regain eligibility after January 1, 2024. These lapses
LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
6
could have a negative impact on health outcomes
for the affected population and also would create
additional administrative workload—first to convert
them to restricted-scope coverage when they
lose eligibility upon aging out and then to re-enroll
them in full-scope coverage once the expansion
is implemented.
Administration States That Earlier
Implementation Could Create Workload
Challenges. The administration has stated
that, due to competing workload, implementing
the proposed expansion any sooner than
January 1, 2024 would be difficult. The competing
workload largely is attributed to the following:
• Conversion to the California Statewide
Automated Welfare System (CalSAWS).
Eighteen counties plan to convert to
CalSAWS (a statewide system to manage
eligibility and enrollment data across various
public benefit programs) between October
2022 and October 2023. In addition to this
process increasing administrative workload
temporarily, updating CalSAWS to reflect
changes in Medi-Cal eligibility policies is
challenging, such that carrying out eligibility
policy changes while the information
technology systems changes are taking place
could result in information being inaccurate in
one or both systems due to a need to rely on
manual processes.
• Resumption of Eligibility Redeterminations.
In addition, during the national COVID-19
public health emergency, the federal
government effectively prohibits terminating
Medi-Cal coverage for existing beneficiaries
except in limited circumstances. After the
public health emergency ends, counties will
need to complete eligibility redeterminations
for the entire Medi-Cal caseload (which
we estimate could be at about 14.9 million
enrollees depending on the end date of the
public health emergency) and end coverage
for any enrollees who are no longer eligible
for Medi-Cal.
• Implementation of Full-Scope Medical
Expansion to Undocumented Residents
Aged 50 or Older. As was noted previously,
undocumented residents who are aged 50 or
older will become eligible for full-scope
Medi-Cal beginning May 1, 2022. Doing an
additional expansion within a short time frame
potentially could complicate work associated
with the 50-and-older expansion, as it affects
the training of eligibility workers and outreach
provided to potential beneficiaries.
We acknowledge that similar to past expansions,
implementing this proposal likely would result in
a temporary increase in administrative workload,
largely for counties due to their key role in
Medi-Cal eligibility administration. While counties
would be facing additional workload demands
simultaneously, we suggest the Legislature
consider alternative strategies for implementation.
Incremental Approach Could Expand
Coverage Faster and Partially Reduce
Workload Impacts. While we recognize that the
workload challenges of an earlier expansion than
that proposed by the administration could be
impactful, they are not necessarily insurmountable.
Notably, the Legislature could take a more
incremental approach to the expansion that
could reduce, although not fully eliminate, some
of the workload challenges noted previously.
For example, the Legislature could take steps to
prevent lapses in full-scope coverage for young
adults who would age out of coverage prior to
January 1, 2024. Two potential approaches would
include (1) directing counties to maintain full-scope
coverage for enrollees who would otherwise be
moved to restricted-scope coverage due to their
age or (2) expanding coverage to people up to
age 30 ahead of the broader January 1, 2024
expansion date. (The latter option would extend
eligibility to people who would otherwise lose
eligibility due to turning 26 after the start of the
national COVID-19 public health emergency in
2020, when eligibility terminations were suspended
and prior to January 1, 2024, when the proposed
expansion would be implemented.)
Recommendation
To the extent the Legislature is interested in
adopting an accelerated time line for all or part
of the population impacted by this proposal, we
recommend that the Legislature request that
the administration provide information about
www.lao.ca.gov
2022-23 BUDGET
7
the feasibility, administrative cost, and caseload
impact of adopting an alternative approach to
implementation. (The Legislature also might seek
similar input from counties due to their key role
in Medi-Cal eligibility administration.) Potential
alternatives could, but do not necessarily need
to, include the options raised above to prevent
coverage lapses for undocumented residents who
are currently enrolled in full-scope Medi-Cal but,
due to their age, would lose their coverage while
waiting for the proposal to be implemented.
REDUCE MEDI-CAL
PREMIUMS TO ZERO COST
Background
Certain Medi-Cal Enrollees Must Pay
Premiums to Be Enrolled in Medi-Cal. The vast
majority of California’s Medi-Cal enrollees do
not pay premiums. However, state residents with
certain characteristics and who have incomes
above standard Medicaid thresholds may
enroll in Medi-Cal provided they pay premiums.
Figure 4 provides more details on the specific
groups of state residents who may enroll in
Medi-Cal with premiums, as well as the amount of
premiums they pay. Populations that potentially can
enroll in Medi-Cal with premiums despite otherwise
not being income-eligible include children,
pregnant women, and persons with disabilities who
are employed.
Reduce All Medi-Cal Premiums to $0.
The Governor proposes to reduce all Medi-Cal
premiums to $0 beginning July 2022.
The administration estimates that this would cost
$18.9 million General Fund ($53.2 million total
funds) in 2022-23, increasing to $31 million General
Fund ($89 million total funds) ongoing.
Assessment
Proposal Would Help Improve Affordability
and Access. Reducing premiums to zero would
help reduce health care costs for the impacted
populations who are relatively low income. It also
could help to improve coverage among people
who are otherwise qualified for these programs
but are not enrolled. First, research shows that
premium costs deter enrollment—including in
similar programs. As such, reducing premiums
to $0 should remove any deterrent effect of the
current premiums. Second, because failure to pay
premiums can result in people being disenrolled
from Medi-Cal, this proposal likely would result in
fewer people losing Medi-Cal coverage.
Fiscal Impact of Potential Increase in
Caseload Is Lacking in Administration’s Cost
Estimate. The administration has stated that it
expects any caseload impacts of the premium
reductions would be minor and difficult to predict.
As such, they do not estimate a caseload impact
from the proposed policy change, nor any
associated costs. However, because the proposal
would remove the deterrent effect of premiums and
reduce the number of people who are disenrolled
from Medi-Cal for not paying premiums, we think
that there is a high likelihood there would be at
least some impact on caseload. While there is
considerable uncertainty about the caseload
impact and corresponding costs, we think these
costs could be in the tens of millions of dollars
General Fund.
Figure 4
Medi-Cal Populations Currently Required to Pay Premiums
Demographic Group FPL Income Range
a
Estimated Caseload Monthly Premium
Children ages 1 through 18 161% - 266% 504,000 $13 per child, $39 family max
Children ages 0 through 1 267 - 322 2,000 $13 per child, $39 family max
Children 0 through 18 in select counties
b
267 - 322 9,000 $21 per child, $63 family max
Pregnant or postpartum persons 214 - 322 6,000 1.5 percent of income
Working persons with disabilities 139 - 250 15,000 From $20 to $250 per person
c
a
Generally counted as household income.
b
Counties include San Francisco, San Mateo, and Santa Clara.
c
Amounts reflect premiums for an individual rather than for a couple and vary based on income.
FPL = federal poverty level.
LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
8
Unclear How Policy Would Impact Potential
Enrollees Who Owe Backpay. At the time of this
analysis, how the proposal would impact potential
enrollees who owe past-due premiums is unclear.
If left unaddressed, these enrollees would still need
to pay the past-due premiums before they can
re-enroll in Medi-Cal, even after premiums have
been eliminated.
Recommendation
Request Additional Information Before
Approving. Due to the potential impact this could
have on improving access and affordability for
low-income Californians, we agree with the policy
basis for the proposal. However, before approval,
we recommend that the Legislature ask the
administration why their assumption of no caseload
impact is reasonable and how past-due premiums
would be handled. This information will be key to
fully understanding both the budget and policy
implications of the proposal—and to determining
whether the proposal should be approved as is
or with modifications to the cost estimates and/or
trailer bill language.
ESTABLISH OFFICE OF
HEALTH CARE AFFORDABILITY
In this section, we (1) provide additional
background on how overall health care costs have
grown in California over time, (2) give context to
efforts in recent years to establish the state Office
of Health Care Affordability to control rising overall
health care costs, (3) describe the Governor’s
proposal to establish—through budget-related
legislation and an associated re-appropriation
of funds—an Office of Health Care Affordability
housed within the Department of Health Care
Access and Information (HCAI) to control health
care cost growth, and (4) provide issues for
legislative consideration regarding this proposal.
Background
Health Care Costs in California Generally
Have Grown Significantly Over Time. Increases
in both health care prices and utilization of health
care services generally have led to higher health
care costs over time. (For example, there was
substantial growth in health insurance premiums
for employer-sponsored health plans of nearly
80 percent—or roughly 4.7 percent per year—
between 2000 and 2017.) For comparison, inflation
in the price of nonmedical services grew by roughly
4 percent per year in both Greater Los Angeles and
the Bay Area over the same time period.
To some extent, health care—like other parts of
the service sector—is structurally predisposed to
greater growth in costs. (For example, the inflation
in nonmedical service sectors discussed above
is still higher than overall inflation over the same
time period.) Nevertheless, growth in health care
costs is attributed at least in part to distinctive
market conditions that particularly impact health
care prices such as reduced competition among
health care payers and providers due to mergers
and acquisitions in the health care sector. As
discussed earlier, these increased health care
costs have led to Californians foregoing or deferring
needed medical care.
Some States Have Created Entities to
Control Health Care Costs. One approach to
controlling health care cost growth is to establish
a regulatory body or independent entity tasked
with implementing a strategy for doing so.
To achieve the goal of controlling health care cost
growth, these regulatory bodies or independent
entities could perform several functions, such as
(1) collecting detailed financial information from
a comprehensive set of health care payers and
providers, (2) providing incentives to encourage
health care payment models based on the quality of
care provided rather than strictly costs, (3) setting
targets for health care cost growth, and (4) levying
penalties on health care entities that do not meet
health care cost growth targets. Some states—
including Massachusetts, Maryland, Rhode Island,
and Oregon—have created entities that perform
some or all of the cost control functions described
above. The efforts implemented in Maryland, Rhode
Island, and Oregon are relatively new. Accordingly,
a comprehensive picture of how effective they have
been at controlling health care costs in these states
is not available. However, the independent entity
in Massachusetts has been in place since 2012.
In the decade since, Massachusetts stayed within
its state health care cost growth targets for the first
several years of implementation. However, it has
exceeded its growth targets in two consecutive
years since then.
www.lao.ca.gov
2022-23 BUDGET
9
Prior Efforts to Create Office of Health Care
Affordability Were Either Delayed or Stalled.
The Governor first proposed the establishment of
an Office of Health Care Affordability—to be housed
in the California Health and Human Services
Agency (CalHHS)—in the January 2020 budget.
This proposal subsequently was withdrawn after
the onset of the COVID-19 pandemic. However, the
2020-21 budget package included budget-related
legislation authorizing the establishment of the
Health Care Data Payments Program (HPD).
The HPD—currently housed within HCAI—is
intended to function as a large research database
derived from individual health care payment
transactions. When it comes online in 2023, the
database will be used to analyze total health
care expenditures statewide to identify key cost
drivers and inform recommendations on how to
mitigate rising costs. The HPD is envisioned as
a key component of the Office of Health Care
Affordability. The Governor’s January 2021 budget
re-proposed the establishment of the Office of
Health Care Affordability, to be housed instead
within the Office of Statewide Health Planning and
Development (later reorganized and reconstituted
into HCAI). In addition to the Governor’s
January 2021 proposal, there was (and remains)
a legislative proposal to establish this office
being considered in the policy process. While no
budget-related or policy legislation has been
enacted to establish the office, the 2021-22 budget
did include an appropriation of $30 million one-time
General Fund to establish the office.
Proposal
Establish Office of Health Care Affordability
Through Budget-Related Legislation.
The Governor re-proposes establishing the Office
of Health Care Affordability within HCAI (through
the enactment of budget trailer bill legislation).
To fulfill its goal of controlling statewide health care
costs, the office broadly is intended to increase
health care price and quality transparency,
develop specific strategies and cost targets for
different health care sectors, and impose financial
consequences on health care entities that fail to
meet these targets. The office would rely heavily
on data collected by the HPD to analyze key trends
in health care costs to identify underlying causes
for health care cost growth (including by reviewing
mergers and acquisitions in the health care
sector). It also would publicly report total health
care spending and factors contributing to health
care cost growth, and publish an annual report
and conduct public hearings about its findings.
In addition, the office broadly would encourage the
adoption of health care payment models based on
the quality of care provided, as well as monitor the
effects of health care cost targets on the health
care workforce.
Within the office, the Governor also proposes
to establish a Health Care Affordability Board
composed of eight members, as follows:
• Four members appointed by the Governor and
confirmed by the Senate.
• One member appointed by the Senate
Committee on Rules.
• One member appointed by the Speaker of
the Assembly.
• The CalHHS Secretary or their designee.
• The Chief Health Director (or their deputy) of
the California Public Employees’ Retirement
System (as a nonvoting member).
The proposed board would be charged with
key implementation decisions for the office.
For example, it would be tasked with approval of the
office’s health care cost targets.
Proposed Statutory Language Includes
Several Revisions to Prior-Year Proposal.
The Governor’s proposed statutory language to
implement the Office of Health Care Affordability
includes several revisions compared to the
administration’s proposal last year. These revisions
include, for example, (1) changes to the size of
the internal board (from 11 members in last year’s
proposal to 8 members in the current proposal),
(2) the addition of authority for the affordability
board—rather than the HCAI director—to approve
health care cost targets, (3) the addition of
certain conditions under which cost targets
could be adjusted for health care entities that
demonstrate substantial growth in labor costs,
(4) updates to financial information required to be
collected (to include nonclaims based payments),
(5) additions of exemptions for provider groups of
LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
10
certain sizes from the office’s requirements, and
(6) modifications to the type of financial statements
that would be accepted by the office (to include
unaudited statements).
Re-Appropriate $30 Million General Fund One
Time for Establishment of Office. The Governor
proposes to re-appropriate the $30 million General
Fund one time to establish the Office of Health
Care Affordability provided in the 2021-22 budget.
This amount is intended to fund the first two years
of implementation of the office. The 2021-22 budget
assumed that the General Fund eventually would
be reimbursed for this cost by the California Health
Data and Planning Fund, which is supported by
fee revenues collected from health care facilities.
This special fund is intended to support the ongoing
costs of the office.
Legislative Proposal to Establish Office Will
Be Revised to Mirror Governor’s Proposal.
As discussed earlier, there also is a legislative
proposal to establish an Office of Health Care
Affordability currently being considered in tandem
with the Governor’s proposal. We understand that
it is the author’s intent is to modify this proposal to
mirror the Governor’s proposal, so this will be the
single proposal for legislative consideration.
Assessment
In Concept, Creating the Proposed Office
a Reasonable Yet Ambitious Step Toward
Controlling Health Care Cost Growth
Statewide… Establishing an Office of Health Care
Affordability—tasked with collecting comprehensive
financial information from across the health care
sector, resourced with the internal expertise
necessary to analyze the data it collects, and
empowered to enforce targets for health care cost
growth—would be a reasonable step for the state
to take in an effort to control health care costs.
However, this proposal also is quite ambitious.
Due to its geographic size, population, and regional
diversity, California’s health care system—and its
total health care spending—is much larger and
more complex than those of the other states that
have attempted to establish independent entities
or regulatory bodies to control health care costs.
Accordingly, carrying out the office’s core functions
may be more challenging than it has been in other
states. In addition, although other states—in
particular Massachusetts—have established similar
models to control health care costs, these efforts
generally do not have a clear and consistent track
record of success. To some extent, this proposed
office will need to develop its own best practices to
ensure that health care cost growth remains within
the specified targets.
…But Continued Monitoring of
Implementation Necessary to Ensure Office
Achieves Goals. In light of the considerations
we raise above, continued monitoring of the
implementation of the Office of Health Care
Affordability would be necessary to ensure it
is successful at controlling health care costs
statewide. This would allow the state to identify
areas where adjustments to the office—such as in
its staffing levels and regulatory authority—would
increase the likelihood that it would achieve its
intended goals.
Issues for Legislative Consideration
Consider Where Further Adjustments to
Proposal Are Needed to Address Legislative
Priorities. As discussed earlier, the Governor’s
proposal includes a number of changes relative
to last year’s proposal. The Legislature may wish
to ask the administration to explain the rationale
for these changes and then consider the extent to
which it agrees with the changes to the proposed
office. If it does not agree with all or some of
the revisions relative to last year’s proposal, the
Legislature may wish to make its own adjustments
to the proposed statutory language to establish
the office.
Consider Putting a Regular Process in
Place to Ensure Legislative Oversight of
Implementation Given continued monitoring
of implementation for this office is warranted
(if enacted), the Legislature may wish to consider
putting a process in place to ensure legislative
oversight of its implementation and ongoing efforts.
The proposed statutory language to establish the
office broadly requires that the Office of Health Care
Affordability be responsive to legislative requests
for information and testimony. Given the ambitious
nature of this proposal, the Legislature may wish
to consider creating a more defined process to
www.lao.ca.gov
2022-23 BUDGET
11
carry out its oversight functions. This could include
requiring regular check-ins, such as on a biannual
basis, with the administration to gain information on
how implementation is going.
REDUCE THE COST OF INSULIN
THROUGH STATE PARTNERSHIP
Background
Addressing High Pharmaceutical Costs
Has Been a Key Priority of the Governor and
Legislature. High pharmaceutical costs have been
identified as a concern of both the Legislature and
Governor. These costs have been attributed to a
variety of factors, including a lack of competition
within the pharmaceutical industry. The state has
taken a number of efforts to address prescription
drug costs. For example, the Governor signed
executive orders in 2019 directing various actions
to address high pharmaceutical costs. These
orders included directing the state to (1) expand
a statewide bulk purchasing program to include
nonstate entities such as local governments and
(2) transition the Medi-Cal pharmacy services
benefit from managed care to fee for service (a
change now known as “Medi-Cal Rx”) in order to
achieve state savings and standardize the Medi-Cal
pharmacy services benefit. In 2020, the Legislature
passed Chapter 207 of 2020 (SB 852, Pan) which
authorized efforts to expand the state’s role
in securing lower cost drugs for Californians.
Specifically, SB 852 directed CalHHS to enter
into partnerships resulting in the production or
distribution of generic prescription drugs with the
intent of making these drugs widely available to the
public and private purchasers.
SB 852 Includes Criteria to Ensure
Partnerships Are Viable and Able to Achieve
Established Goals. Senate Bill 852 requires
that before a partnership is entered into, CalHHS
must (1) only enter into a partnership to produce a
generic prescription drug at a price that results in
savings, targets failures in the market for generic
drugs, and improves patient access to affordable
medications, and (2) examine the extent to which
legal, market, policy, and regulatory factors could
impact the viability of the proposed partnership.
In addition, SB 852 requires reporting by the
administration regarding the potential impacts and
feasibility of a partnership. First, by July 1, 2022,
SB 852 requires the administration to report on
its findings related to the status of drugs being
targeted and how state efforts could impact
competition, access to drugs, and their costs.
Second, by July 1, 2023, SB 852 requires the
administration to produce a report on the feasibility
of directly manufacturing and selling generic drugs.
Governor’s Forthcoming Proposal
The Governor has announced a forthcoming
proposal for a potential partnership to manufacture
insulin. The stated intent is to increase the
availability of insulin that is priced at a fraction
of current market prices. According to the
administration, more detail on this proposal will be
released in the spring.
Assessment
Insulin Could Be an Appropriate Focus for
a Partnership… Insulin costs have increased
substantially over the last two decades. Currently,
even with insurance, patients can end up paying
thousands of dollars in annual out-of-pocket
costs for insulin. In addition, the production
of insulin is heavily dominated by a handful of
companies. Due to the high prices and market
consolidation, a state partnership to produce and
distribute generic insulin has the potential to be
an appropriate focus under SB 852. Moreover,
SB 852 explicitly requires that at least one
partnership the state enters into shall be for the
production of insulin, provided that there is a
viable pathway to manufacturing a more affordable
form of insulin and that the partnership meets the
SB 852 criteria previously discussed.
… But Uncertainty Remains Regarding
Whether Proposal Would Meet SB 852 Criteria
for Viability and Other Factors. While the
proposed partnership has the potential to be
an appropriate focus, whether the partnership
would meet the criteria under SB 852 is unclear.
As noted earlier, SB 852 requires the administration
to examine legal, market, policy, and regulatory
factors that could impact the viability of the
proposed partnership. While the administration

LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
12
notes that these efforts are underway, they have
not yet been completed. In addition, if the state
ultimately would be able to produce generic insulin
at a price that results in savings and improves
patient access to affordable medication as required
by SB 852 remains unclear.
Reporting Required by SB 852 Likely Critical
to Assessing Feasibility of the Proposal.
As noted earlier, SB 852 requires the administration
to report on both (1) its findings related to the
status of drugs being targeted and how state
efforts could impact competition, access to
drugs, and their costs, and (2) the feasibility of
directly manufacturing and selling generic drugs.
This reporting (which is due later in 2022 and 2023)
likely would be critical to assessing the feasibility
of the proposal. As such, why the administration
appears to be moving forward with this proposal
ahead of this reporting is unclear.
Recommendation
Withhold Any Necessary Approvals Until
Additional Information Provided. While we
acknowledge that a partnership to produce
and distribute insulin has the potential to be
an appropriate partnership under SB 852, we
recommend that the Legislature hold off on
approving the proposal until information is provided
to ensure that the proposed partnership meets the
criteria included in the legislation. This information
should include (1) an evaluation of legal, market,
policy, and regulatory factors that could impact
the viability of the partnership, and (2) whether the
state would be able to produce generic insulin at a
price that results in savings and improves patient
access to affordable medication. The Legislature
also might want to consider awaiting the legislative
evaluation of the reporting required by SB 852
before providing the authority to the administration
to enter into any partnerships.
OPTIONS TO IMPROVE
COVERED CALIFORNIA AFFORDABILITY
During last year’s budget process, the
Legislature directed Covered California to
develop options, for consideration during the
2022-23 budget process, to improve affordability
for Californians who have purchased health
insurance through Covered California and make
up to 400 percent of the federal poverty level
(FPL). On January 10, 2022, Covered California
released a report with affordability options for
consideration by the administration and Legislature.
At this time, there are no budget proposals
before the Legislature regarding these options.
The administration has stated that it is still reviewing
the options. As such, if the administration decides
to propose affordability options for Covered
California, the proposal would be later in the budget
cycle. Regardless of whether the administration
ultimately comes forward with a proposal, the
Legislature could consider the options in the
Covered California report and decide whether to
take action regarding the affordability of plans
offered through Covered California.
Background
Federal Patient Protection and Affordable
Care Act (ACA) Substantially Changed
Individual Health Insurance Market Landscape.
The ACA—most of the provisions of which became
effective in 2014—brought about significant
changes to the way that health insurance coverage
is provided in California. This included significant
changes within the individual health insurance
market. Notably, the ACA provided for the
establishment of state health benefit exchanges,
such as Covered California. Consumers who shop
for coverage on Covered California can choose
among health insurance plans organized into
standardized metal tiers, including bronze, silver,
gold, and platinum. These tiers vary in the amount
of monthly premiums they charge and out-of-pocket
costs they require households to pay, such as
annual deductibles and co-pays for medical visits.
Bronze plans have the lowest premiums but have
the highest out-of-pocket costs. For example,
bronze plans feature a large deductible that
www.lao.ca.gov
2022-23 BUDGET
13
must be met before many medical services are
covered. Silver, gold, and platinum plans require
progressively lower out-of-pocket costs, but also
come with higher premiums.
To improve affordability, the ACA created two
types of subsidies that work together to reduce
the cost of health insurance for households who
purchase coverage through Covered California
if they meet certain income-eligibility criteria
and do not otherwise have access to affordable
coverage—such as through an employer, Medi-Cal,
Medicare, or another qualifying program. (The
federal government currently considers coverage
to be affordable if self-only premium costs [that is,
excluding other family members] are no higher than
9.6 percent of household income.)
• Advance Premium Tax Credit (APTC).
The APTC—as structured under the ACA—
offsets the cost of health insurance premiums
for households with incomes between
100 percent and 400 percent of the FPL.
This tax credit effectively limits a household’s
net premium for a silver plan (after accounting
for the tax credit) to between 2 percent and
10 percent of annual income. (This percentage
increases as income increases.)
• Cost-Sharing Reductions. While the
APTC offsets premium costs, cost-sharing
reductions are subsidies that reduce
households’ out-of-pocket costs such
as co-pays, deductibles, and annual
out-of-pocket maximums. Under the initial
years of the ACA, the federal government
provided funding for cost sharing reductions
for insurers in Covered California to offer
various “enhanced” silver plan options
to households with incomes between
100 percent and 250 percent of the FPL.
These plans are often referred to by the
average percent of a member’s health care
costs that the plan pays. For example, on
average, a Silver 94 plan pays 94 percent
of member health care costs. Plans with
higher numbers—which have a lower income
threshold for enrollment—are considered
more generous because the consumer pays
lower out-of-pocket costs. In 2017, the federal
government stopped providing funding for
cost-sharing reductions but did not remove
the requirement for insurers to offer enhanced
silver plans that included cost-sharing
reductions. In order to accommodate the
increased cost of silver plans, insurers raised
premiums for silver plans. (We note that due to
the APTC, the federal government ultimately
paid for the increased premium costs for
consumers making less than 400 percent
of the FPL.)
ACA Created Individual Mandate That Was
Subsequently Set to Zero. As originally enacted,
the ACA imposed a requirement, referred to as the
individual mandate, that most individuals obtain
specified minimum health insurance coverage or
pay a penalty. The individual mandate was intended
to discourage people from going without health
insurance coverage, particularly younger and
healthier individuals who have lower risk of incurring
health care costs and who otherwise would be less
likely to enroll in coverage. Increased coverage
of younger, healthier populations leads to a more
balanced insurance risk pool and allows the costs
of covering higher-risk populations to be spread
more broadly. This, in turn, reduces the average
cost of coverage and helps to offset the increased
cost of making individual market coverage more
comprehensive under the ACA. However, due to
subsequent federal legislation, the penalty for
violating the individual mandate has been reduced
to zero, effectively eliminating the requirement.
State Introduced Individual Mandate Penalty
and Established Three-Year Premium Subsidy
Program. In 2019-20, the Legislature enacted
a state individual mandate penalty as well as a
three-year state premium subsidy program intended
to supplement federal subsidies through Covered
California. The state’s individual mandate penalty,
which was modeled on the federal individual
mandate penalty, went into effect in 2020 and is
ongoing. The subsidy program was designed as a
three-year program from 2020 through 2022 that
would reduce premium costs for most Covered
California enrollees—including those making
between 400 percent and 600 percent of the
FPL who were not eligible for the federal premium
subsidies. The state subsidies were structured
to limit premium costs to a percentage of income
(with the percentage increasing with income) for
households making up to 600 percent of the FPL.
LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
14
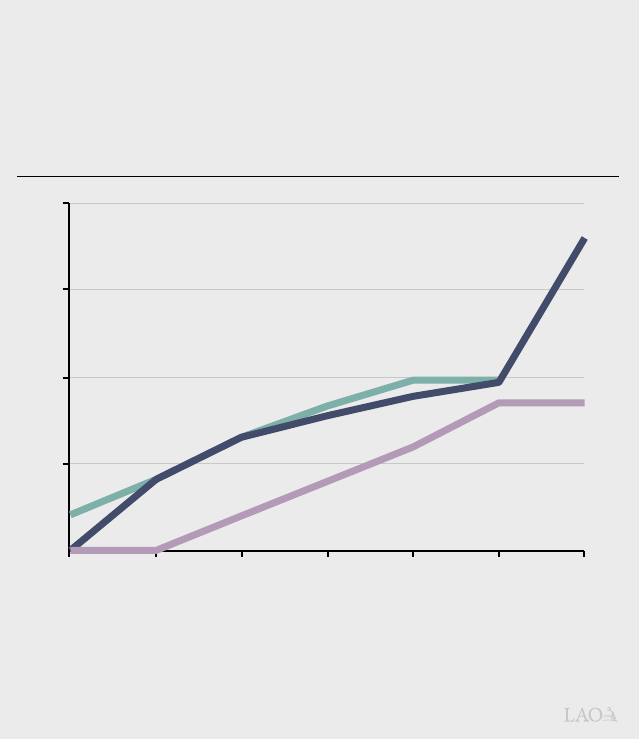
Enhanced Federal Premium Subsidies in
Effect Supplanted State Subsidies in 2021
and 2022. The American Rescue Plan (ARP) Act
was passed by Congress in 2021 in response to
COVID-19. As part of this act, the level of federal
support for premium subsidies for coverage
purchased on health benefit exchanges have
been temporarily increased for the 2021 and 2022
plan enrollment years. As seen in Figure 5, the
increased federal premium subsidies substantially
lower the cost of premiums Californians need to pay
for plans purchased through Covered California—
including for households whose incomes made
them ineligible for the preexisting premium
subsidies under the ACA. In total, the increased
federal support has resulted in about $1.6 billion in
reduced premium costs for Californians annually in
each of 2021 and 2022.
State Set Aside Funding for Future
Affordability Program and Required Report
on Affordability Options.
The increased federal support
effectively supplanted the state
premium subsidies because it
reduced premium costs as a
percent of income below the
thresholds established in the state
program. This freed up General
Fund that otherwise would have
gone toward the state premium
program. As part of the 2021-2
budget package, Chapter 143 of
2021 (AB 133, Committee on
Budget) set aside $333.4 million
of this freed-up General Fund
to support future affordability
efforts. Assembly Bill 133 also
required Covered California to
develop options for reducing
out-of-pocket costs for enrollees
making up to 400 percent of
the FPL and to provide these
options to the Legislature and
Governor for consideration in the
2022-23 budget process.
Pending Federal Legislation Could Extend
ARP Act Premium Subsidies and Provide
Additional Cost-Sharing Reductions. As noted
above, the increased federal support through the
ARP Act only extends through 2022. However,
pending federal legislation (referred to as the Build
Back Better Act) would extend the increased
federal support through 2025. The legislation also
would provide a total of $10 billion nationwide
annually between 2023 and 2025 to support new
cost-sharing reductions. (The likelihood of the
pending federal legislation—or legislation with
similar provisions—ultimately being approved by
Congress is highly uncertain at this time.)
Affordability Remains an Issue for
Households With High Out-of-Pocket Costs.
Even with the federal premium subsidies and
the cost-sharing reductions established through
the ACA, affordability remains an issue for both
low-income consumers who are eligible for plans
20%
a
Because individuals with incomes below 138 percent of the FPL generally are eligible for Medi-Cal, Californians
below this income level rarely, but sometimes, receive subsidized coverage through Covered California.
b
Federal subsidies were not previously available for individuals with incomes over 400 percent of the FPL.
Eligibility for the California state subsidy program ends at 600 percent of the FPL, while the ARP has no such
income limit for eligibility.
ARP = American Rescue Plan and FPL = federal poverty level.
Figure 5
ARP Reduced Premium Costs in Covered California,
Supplanting State Premium Subsidies
Maximum Required Contribution Toward Silver Plan Premiums as a
Share of Income by FPL Group
10
5
15
Under
138
a
138-
150
150-
200
200-
250
250-
300
300-
400
Over
400%
b
Preexisting Federal Subsidies
(Ongoing)
State Subsidy Program
(Expires December 31, 2022)
ARP Subsidies
(Expires December 31, 2022)
www.lao.ca.gov
2022-23 BUDGET
15
that include the ACA cost-sharing reductions as
well as higher-income households. As shown in
Figure 6, households at various income levels
who are enrolled in silver plans potentially can end
up paying a high percent of their annual income
on health expenditures. For example, a family of
four making about $40,000 per year and enrolled
in an enhanced Silver 87 plan (with cost-sharing
reductions) could end up paying $5,700 out of
pocket (over 14 percent of their income) over the
course of a year and potentially within a much
shorter period of time. A four-person household,
making roughly $67,000 per year and enrolled in
a standard Silver 70 plan (with no cost-sharing
reductions) could end up paying $16,400 (almost
24 percent of their income) in out-of-pocket costs
over the course of a year.
Recent Report Provides Various
Options to Improve Affordability
Report Highlights Various Options to Improve
Affordability. On January 10, 2022, Covered
California released a report with various options for
cost-sharing reductions to improve affordability for
silver plans purchased through Covered California
in response to AB 133’s reporting requirement.
These options are laid out in more detail in Figure 7
on the next page, but generally involve eliminating
deductibles (which are primarily assessed for
inpatient services) and providing at least some
portion of enrollees with more “generous” plans
than they would otherwise qualify for—which would
reduce out-of-pocket costs. (The generosity of a
plan refers to the percentage of a member’s health
care costs that it is assumed to cover.) At this time,
the administration has not put forward a proposal
regarding these options.
Funding Issues
Affecting Affordability Options
The section below discusses some issues for
legislative consideration regarding potential changes
in the amount of federal funding available to improve
affordability in Covered California and other potential
sources of funding.
Will Federal Support for Premium Subsidies
in ARP Act Be Extended? As noted earlier, pending
federal legislation potentially would extend the federal
support for enhanced premium subsidies provided
through the ARP Act through 2025. However, if the
enhanced premium subsidies are not extended and
the state took no action in response, this would result
Figure 6
Silver Plan Out-of-Pocket Maximums as a Percent of Annual Household Income
Family of Four, 2022
5
25%
Annual Household Income (In Thousands)
$5,700
$12,600
$16,400
Out-of-Pocket Maximum
15
10
20
$1,600
40 50 60 70 80 90 10045 55 65 75 85 95 $105

LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
16
in a substantial increase in premium costs for
households enrolled in Covered California.
Covered California noted in its report that if
faced with increased premiums, thousands
of existing enrollees might choose to drop
coverage. In the event the federal premium
subsidies under ARP are not extended,
the Legislature may wish to consider
reestablishing a state premium subsidy
program before considering adopting
state-funded cost-sharing reductions (such
as the options provided in the Covered
California report) due to the potential adverse
impact increased premium costs could have
on affordability and thus access to coverage.
Will the Federal Government Provide
Funding for Cost-Sharing Reductions?
The pending federal legislation would
provide $10 billion in federal funding
for additional cost-sharing reductions.
California’s share could potentially exceed
$1 billion, although the amount of funding
and level of discretion provided to the state
remains uncertain. In the event this funding is
approved, the state would have considerably
more resources to address affordability of
plans provided through Covered California.
However, the Legislature would need to
take into consideration potential federal
requirements on how this funding is utilized.
In addition, the Legislature will want to take
into consideration that even if the pending
federal legislation is approved, the federal
funding for cost-sharing reductions would
only be provided through 2025.
Beyond Federal Funding, What Other
Funding Could Be Used? Aside from
the potential for enhanced federal
funding, the Legislature could choose to
authorize General Fund for the purpose
of implementing affordability options in
Covered California. For example, the
Legislature may wish to spend an amount
similar to the estimated revenues from the
state’s individual mandate penalty for a
state subsidy program. Revenues from the
penalty for the 2020 tax year were about
$400 million.
Figure 7
Summary of Options Presented in
Covered California Report
Options
Estimated State
Fiscal Impact
a,b
Option 1
Households with incomes above 150 percent up to
600 percent of the FPL would be upgraded to more
generous plans.
$475 million to $626 million
All deductibles would be eliminated.
Option 2
Households with incomes above 150 percent up to
400 percent of the FPL would be upgraded to more
generous plans.
$463 million to $604 million
All deductibles would be eliminated.
Option 3
Households with incomes above 150 percent up to
400 percent of the FPL would be upgraded from
existing plans to plans somewhat less generous than in
Option 2.
$386 million to $489 million
All deductibles would be eliminated.
Option 4
Similar to Option 3 but with less generous upgrades for
households with incomes above 250 percent up to
300 percent of the FPL.
$362 million to $452 million
All deductibles would be eliminated.
Option 5
Households with incomes above 150 percent up to
250 percent of the FPL would be upgrade to more
generous plans.
$278 million to $322 million
All deductibles would be eliminated.
Option 6
No change for households at or below 200 percent of the
FPL. Households above 200 percent and up to
400 percent of the FPL would be upgraded to a more
generous plan.
$128 million to $189 million
All deductibles would be eliminated.
Option 7
No change for households up to 250 percent of the
FPL. Relative to Option 6, somewhat less generous
upgrades for households above 250 percent up to
400 percent of the FPL.
$37 million to $55 million
Deductibles would not be eliminated.
a
Estimates provided by Covered California with low to high estimates varying by the extent to which
existing enrollees shift to more generous plans as a result of the option.
b
Estimated costs do not assume any new enrollment resulting from the plans. To the extent options
encourage new enrollment into Covered California, state costs could be higher than listed in the
table.
FPL = federal poverty level.
www.lao.ca.gov
2022-23 BUDGET
17
Other Issues for
Legislative Consideration
Regardless of what sources of funding are used,
we suggest the Legislature consider various other
issues if it chooses to establish a state cost-sharing
reduction program (such as one of the options
provided in the Covered California report). A few
issues for consideration are discussed below.
What Specific Affordability Goals Should Be
Pursued? If the Legislature decides to establish a
cost-sharing reduction program, determining what
specific affordability goals should be pursued will
be important. For example, the Legislature could
focus on improving affordability for lower-income
households who, despite being eligible for
federal cost-sharing reductions, can still pay a
significant portion of their income on health care
due to deductibles and out-of-pocket maximums.
Alternatively, the Legislature could focus on
expanding cost-sharing reductions to households
with incomes above 250 percent of the FPL who
do not currently qualify for federal cost-sharing
reductions and, as a result, potentially could end
paying an even higher percent of their income on
health care.
While Covered California’s report is heavily
focused on affordability for existing enrollees, in
2023, about 700,000 Californians are projected
to be uninsured but eligible for subsidized
Covered California plans while an additional
200,000 uninsured Californians would be eligible
for unsubsidized Covered California plans.
Encouraging these Californians to enroll in Covered
California could significantly reduce the number of
uninsured Californians. Accordingly, the Legislature
might want to focus on affordability options that
promote further take-up of insurance coverage.
While Covered California provides detailed
information about the impacts of its options on
affordability for different income groups, however,
the report does not consider potential impacts the
options would have on enrollment.
What Out-of-Pocket Costs Should a State
Cost-Sharing Reduction Program Address?
The Legislature also may wish to consider what
type of out-of-pocket costs should be focused
on by such a cost-sharing reduction program.
The majority of the options put forward by Covered
California include eliminating deductibles and
providing consumers with more generous plans
that reduce various out-of-pocket costs. Only
one option would provide more generous plans
but would not eliminate deductibles. The options
that eliminate deductibles are considerably
more expensive. However, the Legislature might
want to consider these options for two reasons.
First, inpatient deductibles are substantially higher
than other forms of out-of-pocket costs. While
many consumers do not utilize these services,
those who do are much more likely to reach their
out-of-pocket maximums. Second, deductibles
can have a deterrent effect on consumers. Notably,
if consumers are confused about when such
deductibles apply, they may avoid enrolling in plans
or receiving health care, including services that are
not subject to inpatient deductibles.
Would the Cost-Sharing Reduction Program
Be Limited Term or Ongoing? The Legislature
also may want to consider what duration a
state-funded cost-sharing reduction program
should be. A one-year or limited-term program
would reduce the state’s fiscal exposure and
potentially avoid exceeding the $333.4 million that
was set aside in 2021-22. In addition, if the pending
federal legislation to provide funding for cost
sharing is approved, the associated federal funding
would expire in 2025. As such, a limited-term state
program could be better aligned with that funding
source and later restructured or eliminated when
the federal funding goes away. However, there are
trade-offs of a limited-term program. For example,
consumers may be less willing or able to make any
necessary changes to their health plans in order to
benefit from a program that has a short duration.
Legislative Next Steps
While no specific proposal has been put
forward by the administration, action would
need to be taken within the 2022-23 budget
process in order to take effect in Covered
California’s 2023 plan year. We recommend that
the Legislature take into consideration the issues
raised above when considering what actions to
take—either in reviewing any potential proposal
from the administration that might be released
at May Revision or in developing direction to the
administration on what options to implement.

LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
18
VARIOUS ACCESS AND
AFFORDABILITY ISSUES REMAIN
The Governor’s proposals—if approved by the
Legislature—would improve significantly access to
comprehensive health coverage and to some extent
improve affordability. In addition, potential actions
taken to improve affordability in Covered California
would reduce health costs for impacted households.
However, various issues regarding access to
comprehensive health coverage and affordability of
health care would remain even if the above actions
were all taken. We provide a few notable examples of
these issues below.
Examples of Issues Impacting Access
to Comprehensive Coverage. These access
issues include:
• Access to Covered California for
Undocumented Residents. While the
Governor’s proposal would expand Medi-Cal
coverage to all income-eligible undocumented
residents, access to coverage would remain
an issue for undocumented residents who
are not income-eligible for Medi-Cal. While
there is considerable uncertainty about the
size of this population, we estimate there likely
are 300,000 people affected. Due to federal
requirements, such individuals are excluded
from purchasing coverage through Covered
California. However, the state potentially could
seek a federal waiver to allow such individuals
to purchase coverage. Even with a waiver,
however, costs of plans purchased likely would
either need to be unsubsidized or the state
would need to pay for any subsidies that would
otherwise be funded by the federal government.
• Reducing Number of People Eligible
for but Not Enrolled in Medi-Cal.
Roughly 500,000 people are eligible for but
not enrolled in Medi-Cal, although it is not
necessarily the same 500,000 people at a
given time due to an issue known as “churning.”
Churning refers to when individuals lose
eligibility for Medi-Cal on a temporary basis
before resuming coverage, often within a
year. The lapses in coverage due to churning
can result in issues with continuity of care.
Reasons for churning can be due to short-term
changes in circumstances such as temporary
increases in income, but it also can be due to
administrative issues such as failure to respond
to Medi-Cal eligibility redetermination notices
within a given amount of time. The Legislature
could consider asking the Department of Health
Care Services for other options to streamline
the eligibility redetermination process from
a beneficiary perspective for the purpose of
reducing churn. Alternatively, the Legislature
could consider adopting a continuous coverage
policy to allow enrollees to remain on Medi-Cal
for a period of time, such as a year, without
being subject to an eligibility redetermination
(this would require a federal waiver).
Examples of Issues Impacting Affordability.
These affordability issues include:
• Addressing Share of Costs in Medi-Cal.
Certain individuals who would otherwise not
be eligible for Medi-Cal due to their income are
allowed to enroll in the program but must pay
a share of cost before enrolling in Medi-Cal.
Most share-of-cost Medi-Cal recipients are
enrolled in the medically needy program
which is largely comprised of persons with
disabilities as well as people who are aged or
blind. In contrast to the payment of premiums,
individuals who pay a share of cost must meet
a monthly deductible before Medi-Cal begins to
pay for health care. The amount of deductible
that must be paid each month is calculated as
the enrollee’s net nonexempt income minus
a basic amount determined to be necessary
for cost of living, known as the “maintenance
need level.” California has not applied
cost-of-living adjustments to the calculation of
the maintenance need level since 1989, even
though federal law allows for such adjustments,
resulting in a current maintenance need level
of only $600. Introducing inflation adjustments
into the program could help mitigate increasing
affordability challenges for its enrollees.
www.lao.ca.gov
2022-23 BUDGET
19
• Fixing the “Family Glitch.” Under the ACA,
households that have access to affordable
health insurance through other sources such
as an employer are ineligible for federally
subsidized health plans through exchanges
such as Covered California. Under the ACA,
households are considered to have access to
affordable insurance if at least one member of
the household has access to health insurance
in which the cost of self-only coverage is less
than a certain percent of household income
(currently 9.66 percent). The definition does
not consider the cost of coverage for other
household members and accordingly has
become known as the family glitch because
of its potentially adverse impact on families
being able to access affordable coverage
through the health benefit exchanges. In some
circumstances, such as if an employer
contributes little to nothing for the coverage
of spouses and dependents, households
may find it cost-prohibitive to either add other
family members to an employer-sponsored
plan or purchase nonsubsidized coverage
through Covered California. While this issue
could be addressed through a change in
federal legislation, Minnesota recently passed
legislation to address the family glitch at the
state level. (However, we note that Minnesota’s
equivalent to Covered California is structured
very differently—and as such, attempting to
fix the family glitch in California could require a
different approach and be more complicated.)
• Reducing Pharmaceutical Costs.
This publication discusses the Governor’s
proposal to address high insulin costs. Even
if that proposal is approved and implemented
successfully, high pharmaceutical costs
likely will remain a challenge—even after
considering he state’s other efforts to
reduce such costs. Attempting to address
this issue could require additional market
interventions—such as attempting to increase
competition, consolidating the purchase of
pharmaceuticals to a greater extent than today
to increase bargaining power, or passing
legislation to regulate costs. However, the
feasibility of any such intervention is uncertain
and could lead to unintended consequences,
such as reduced availability if manufacturers
choose to reduce the availability of their drugs
to Californians due these state interventions.
To the extent the Legislature would like to further
the goals of improving access and affordability, it
could consider looking into ways to address the
issues identified above. This could include asking
the administration during budget deliberations
about its plans, if any, to address the issues
identified, as well as about the feasibility of options
to address them. We recognize that options to
address some of these remaining access and
affordability issues may be costly and complicated
and come with significant trade-offs that warrant
serious consideration before proceeding.

LEGISLATIVE ANALYST’S OFFICE
2022-23 BUDGET
20
LAO PUBLICATIONS
This report was prepared by Luke Koushmaro, Ben Johnson, and Corey Hashida, and reviewed by Mark C. Newton
and Carolyn Chu. The Legislative Analyst’s Office (LAO) is a nonpartisan office that provides fiscal and policy
information and advice to the Legislature.
To request publications call (916) 445-4656. This report and others, as well as an e-mail subscription service, are
available on the LAO’s website at www.lao.ca.gov. The LAO is located at 925 L Street, Suite 1000, Sacramento,
California 95814.
